NYU Professor Julia Evergreen Keefer
This is an Anatomy and Kinesiology, not Physiology class. The focus is on the musculoskeletal system in movement, which means we will also study the nervous system that fires it, and the cardiorespiratory system that pumps the blood to nourish the muscles and bones. We will not be going into the details of the urinary, reproductive, endocrine, or digestive systems. In order to distinguish between performance, everyday movement, disease, age, and illness, we will also cover pathology as it related to specific joints and muscles.
Objectives: To learn the form and function of the muscles, joints, and nerves; to study movement patterns in space in terms of physics, in an effort to improve function and design exercise programs that make the transition between physical therapy and performance training.
Requirements:
Weekly quizzes on anatomy/kinesiology based on the textbooks and Professor Keefer's lectures
Weekly lab work to move joints, study pathology, and/or design sport-specific or dance programs
Comparative Case Studies of your choice: midterm progress report and final project
Final Exams, written and practical
Breakdown
Classes meet twice a week, asynchronously online for the lectures, forums, and quizzes, and once a week at the gym for the practicum. Attendance is crucial for this hands-on work. Anatomy doesn't change, kinesiology is always improving, pathology keeps getting worse, but your job is to learn the basics but come up with innovative programs to solve problems based on your chosen case studies.
Week One: Feet and Ankles
Week Two: Knees
Week Three: Hips
Week Four: Lower Back
Week Five: Upper Back and Neck
Week Six: Shoulders
Week Seven: Elbows
Week Eight: Hands
Week Nine: Gait Analysis and Endurance Sports (running, cycling, hiking, skiing)
Week Ten: Ball Sports (trajectories and teams)
Week Eleven: Dance (ballet, modern, jazz, hip hop, Middle Eastern)
Week Twelve: Martial Artists (impact, contact, interaction)
Week Thirteen: Body Building
Week Fourteen: Final Projects Due. Demonstrate case studies.
Links
From Pain to Performance
Lower Body
Upper Body
Before going to Periodization for Performance , you might want to ground yourself with real life aerobics and EvergreenEnergy in Evergreen Fitness for the Four Seasons , or get into great cardio-strength shape at home with Evergreen's Knockout Workouts.
<julia.keefer@nyu.edu> Dr. Keefer is an NYU Professor, a kinesiologist, massage therapist, fitness instructor, and creator of four trademarked classes, (EvergreenEnergy: Stretch, Sculpt and Meditate, Aerobic-Gut-and-Butt, Knockout Step/Slide/Strike, and Knockout Ballet 'n Box). In her private practice, she specializes in rehab and prehab to keep you happy hab with exercise and massage therapy, postural retraining, and ideokinesis. She has worked for a neurosurgeon, a psychiatrist, an osteopath, a vascular surgeon, an orthopedist, and a podiatrist, giving her a head-to-toe knowledge of the human body. A former professional wrestler and dancer/actress, Dr. Keefer understands the pain, perks, parameters, and perfectionism of performance and how to form the bridge between physical therapy and performance training. She also teaches electronic media performance and the Keefer Brain Gymnasium, thereby making the mindbody connections necessary to optimal function.
Notes on Basics for Personal Trainers:
NOTES AND STATS
Summer 2007-07-19
THE NEUROMUSCULAR SYSTEM
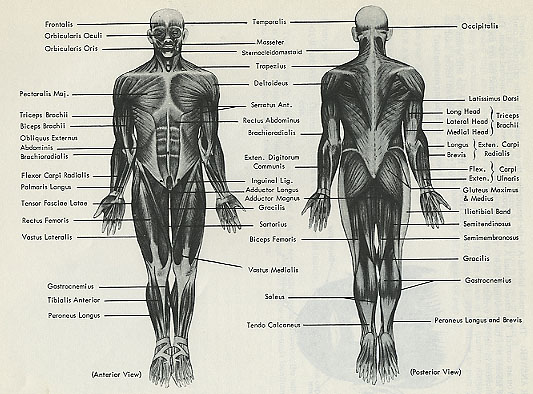
Skeletal muscle is 36% to 45% of total body weight; there are over 600 different muscles, and it is the most plentiful tissue in the body.
Skeletal muscles can be stretched up to 150% of their resting length.
Muscle fiber can be a few millimeters (in the eye) to 30 centimeters (12 inches) in the sartorius, longest muscle in the body.
Type I fibers are fatigue resistant, with a larger number of mitochondria and mitochondrial enzymes, slower calcium capability, lower myosin ATPase, inhibiting speed of hydrolysis of ATP but producing more ATP. Most people possess 45% to 55% slow-twitch fibers in their limbs, although sprinters have more fast-twitch fibers in their limbs.
Type II Fast-twitch fibers generate fast, powerful muscle actions because of speedy calcium release, a high level of myosin ATPase, and a developed sarcoplasmic reticulum. Type IIa or FOG are slow glycolytic, Type IIb, fast glycolytic.
Functional unit of the neuromuscular system is the motor unit, which consists of the motor nerve (cell body, axons (signals away from the cell body), and dendrites (signals to the cell body), covered by a myelin sheath made up of Schwann cells, with gaps every one or two millimeters called the nodes of Ranvier, jumping along in saltatory conduct-ion, sometimes at a speed of 100 meters per second (220 miles per hour!). Vesicles containing neurotransmitters such as acetylcholine, norepinephrine, dopamine etc, lie on axon terminals where they squirt their juice into the synapse, the junction between two nerves, or a neuromuscular junction, between a nerve and a muscle at the motor end plate, to continue an action potential. If the cell membrane's electrical potential changes to a value of -50 to -55 millivolts, it reaches its electrical threshold and will conduct an action potential along the axon to the target muscle or organ. The membrane potential will change from the -70 millivolts to a value of +30 millivolts in an action potential, because sodium ions rush into the cell.
After depolarization, repolarization occurs as potassium ions move to the outside of the cell to regain the -70 millivolt resting membrane potential. Then the sodium-potassium pump restores equilibrium.
Proprioceptors are muscle spindles, (located in intrafusal fibers parallet to extrafusal fibers) Golgi tendon organs, and Pacinian corpuscles (sensory). A sarcomere is the functional unit of the muscle cell that runs from Z-line to Z-line. Within the sarcomeres are thin protein, myofilaments (actin) and thick protein myofilaments (myosin) that have cross-bridges or heads extended from them. Also attached or surrounding the actin myofilaments are tropomyosin and troponin into which the tropomyosin molecules are embedded. Each myosin myofilament is surrounded by six or more actin myofilaments. A sarcomere has a striated appearance due to I-bands that are light areas near the Z-lines consisting of actin myofilaments; A-bands that are dark areas consisting of both actin and myosin myofilaments; and a H-zone that is a slight variation in the shading of the A-band due to the absence of the actin myofilaments.
The Sliding Filament Theory:
Myosin and actin do not change length
Z-lines move closer together
I-band shortens
A-band stays the same length
H-zone disappears
SR contains calcium stores
Events of muscle action: rest, excitation-coupling, (action potential, across synapse, into the interiror via the t-tubules, influx of calcium into the axon terminal signals the rlease of acetylcholine from the axon, binding of calcium on troponin for force production) contaction, recharge, relaxation
Roles of ATP: a) Myosin ATPase pulls off a phosphate from ATP to turn it into ADP, which drives the power stroke of the myosin head; b) Binding of myosin crossbridge heads to actin�power stroke occurs as force is developed; c) ATP is required to actively pump calcium back into the SR to allow movement (release crossbridge). Peak rate ot muscle contraction is dependent on myosin ATPase activity and the size of the motor neuron. Maximal force or tension a muscle can generate is dependent on the amount of actin-myosin binding taking place.Continuation of muscle contraction is dependent on the ability to recycle ATP. Slow twitch are the easiest to stimulate, fast twitch the most difficult. Force production is influenced by number of muscle fibers, size and number of motor units, rate coding, or the frequency of neural impulses, force-velocity curve or the speed of movement and distribution of muscle fiber types, eccentric stronger than concentric. The length of a muscle fiber is related to the overlap of contractile proteins. Pre-stretching fibers to 120% of their normal resting length will optimize force production. Fatigability is due to the duration of the activity, related to fiber type. Size principles�smaller cell bodies are recruited first. The mechanical arrangement of muscles affects force production, pennation, which effects speed of shortening, fiber packing, and altered force and power capacity. Fatigue decreases force production with increased hydrogen ions, decreased pH, reduced energy, reduced calcium release, reduced troponin's sensitivity to calcium.
THE SKELETAL SYSTEM
The skeletal system has over 200 bones in the axial and appendicular portions, made up of 80% compact bone arranged into the Haversian system, designed for support and protection, and cancellous or soft porous bone with trabeculae, good for hematopoiesis and storage of calcium and phosphate. Osteoclasts, osteoblasts, and osteocytes are involved in resorption, formation, and remodeling respectively.
Tendons (muscle to bone) are made up of collagen, an inelastic tissue with great tensile strength consisting of three amino acids in a triple helix, which is the most abundant protein in the body, and ground substances. Ligaments (bone to bone) are made up of collagen and elastin, which permits some extensibility and return to resting length.
There are three types of fascia�superficial, deep, and subserous or fluid-containing, covering internal viscera like the heart�which bind muscle, transmit forces, and insulate organs.
THE CARDIOPULMONARY SYSTEM
(SV) or Stroke Volume is the amount of blood ejected in milliliters by the left ventricle, as a result of end-diastolic volume (amount of blood at end of filling phase) a stretch reflex and the release of catecholamines, or hormones of the sympathetic nervous system to allow for greater systolic emptying of the hear. (Q) or Cardiac Output is the amount of blood pumped by the heart, determined by Stroke Volume times Heart Rate.
Q=SV times HR. The vagus nerve of the parasympathetic system decreases HR. CO is influenced by venous return, end diastolic volume which increases SV, strength of cardiac contraction from sympathetic nerve activity of Frank-Starling principle, parasympathetic to decrease, and mean arterial pressure in the body.CO is distribution to skin and muscles during exercise, but brain and heart remain constant.
The SA node controls rhythm of electrical stimulation of the heart, discharging around 60 to 80 times a minute. ECGs consist of a P wave, a QRS complex, (recordings of the electrical stimulus through ventricular myocardial tissue) and a T wave, which represent atrial depolarization which initiates atrial contraction, electrical recovery following ventricular depolarization.
SPp is the pressure exerted against the arterial walls as blood is forcefully ejected during ventricular contraction or systole. Rate-pressure product, or double product, is the estimate of the work of the heart.
rate-pressure product = HR times SBp
DBp is the pressure exerted against the arterial walls when NO blood is being forcefully ejected through vessels, providing an indication of vascular stiffness or resistance, decreased with vasodilation, increased with vasoconstriction. Blood pressure falls progressively to nearly 0nnHg (millimeters of mercury) by the time it reaches the termination of the right vena cava of the atrium. Hypertension is over 140-90. Aerobic exercise can double this, while Valsalva can triple it.
Mean arterial blood pressure is the average blood pressure throughout the cardiac cycle= [(SBp-DBp) divided by 3] + DBp
Men have about 15-16 grams of hemoglobin per 100 milliliters of blood.
Women have about 14. One gram of hemoglobin can carry 1.34 milliliters of oxygen. Movement of gas across a cell membrane is diffusion, so the concentration gradient results in the exchange of oxygen and carbon dioxide. The oxyhemoglobin dissociation curve describes the impact of increased metabolism on oxygen dissociation, because as blood temperature, concentration of carbon dioxide, and acidity increase with exercise, oxygen more readily dissociates from hemoglobin, and makes itself available.
Only about 5% of carbon dioxide produced during metabolism is transported out of the cell by diffusion and subsequently transported by the plasma to the lungs. 70% results form a process involving CO2 and water in the red blood cells and subsequent delivery to the lungs in the form of bicarbonate.
Oxygen Uptake is the amount of oxygen utilized by the tissues of the body, dependent on cardio output or volume of blood transported, and arteriovenous difference a-v02 difference or the difference in the oxygen content of the arterial blood versus venous blood expressed in milliliters of oxygen per 100 milliliters of blood.
V02=Q times a-V02 difference, where Q equals cardiac output (HR times SV) in milliliters per minute
V02 rest= (80 bests/min times 65ml blood/beat) times 6ml 02/100 ml blood
=312 ml02 min or
VO2 rest= (HR times SV) times a-V)2 difference
To get the usual results for oxygen uptake, ml/kg/min, one then divides the result by the person's weight in kilograms. 312 ml02 divided by 75 kg= 4.2ml 02 kg min.
MOST IMPORTANT EQUATION IS THE FICK EQUATION: Q=V02 divided by a-V02 difference
Q=312ml 02 min divided by 6 ml 02/100 ml blood
=5200 ml/blood/min
=5.2 l blodd/min
Since maximal oxygen uptake is somewhat theoretical, peak oxygen uptake measures an actual measured value subject to change.
Resting oxygen uptake is generally estimated at 3.5ml02 kg/ min, or one metabolic equivalent or MET. Peak oxygen might range from 35 to 80 ml kg min or 10 to 22.9 METs in normal, healthy persons.
Minute ventilation is the volume of air breathed per minute, measured by tidal volume, the amount of air moved during inhalation or exhalation with each breath, times respiratory rate. Inspiratory and expiratory reserve volumes measure the amount of air beyond normal resting tidal volume. Forced vital capacity is the amount of air moved from maximal inspiration and expiration. Residual lung volume is what is left to prevent the lungs from collapsing. The total lung capacity is forced vital capacity and residual lung volume. The normal volume of anatomical dead space in nose, mouth, trachea, bronchi and bronchioles is 150 milliliters in young adults, increasing with age. Physiological dead space refers to alveoli with poor blood flow, poor ventilation, disease etc. At rest the partial pressure of oxygen in the alveoli is about 60 mmHg greater than in the pulmonary capillaries, to allow diffusion into the lungs. Similarly C)2 diffuses in the opposite direction. Expired ventilation rate, carbon dioxide production rate, and lactic acid production from glycolysis increase exponentially (curvilinear) as workload increases up to max, while oxygen uptake and heart rate tend to increase linearly.
The pons and medulla oblongata control dorsal (initiation and rhythm) and ventral respiration (increased ventilation, inspiration, forceful expiration. Pneumotaxic center controls rate and pattern of breathing.
Effects of training: Expired ventilation rate, carbon dioxide production rate, and oxygen uptake are higher during maximal exercise, decreased during submaximal because of efficiency, and no change at rest, although resting heart rate may go down.
BIOENERGETICS
Energy substrates are phosphagens (ATP and creatine phosphate), glucose, glycogen, lactate, fatty free acids, and amino acids. Creatine phosphate can decrease 50% to 70% during the first 5-30 seconds, and be almost eliminated with very intense exercise. Muscle ATP concentrations do not decrease by more than about 60% from initial values. Postexercise phosphagen repletion can occur in a short period; complete resynthesis of ATP appears to occur within 3 to 5 minutes; and complete creatine phosphate resynthesis can occur within 8 minutes, largely as a result of aerobic metabolism. About 300 to 350 grams of glycogen is stored in the body's total muscle, and about 70 to 100 grams in the liver, which can increase with training. About 60% of VO2 max, muscle glycogen is an important energy substrate, and it can be depleted during intense exercise, and can be the limiting factor for heavy resistance training with multiple sets. Repletion appears to be optimal if 0.7 to 3.0 gram of carbohydrate per kilo is ingested every two hours following exercise. High eccentric components may take more than 24 hours to replete.
ATP is composed of adenine, ribose, three phosphate groups, breaking down to adenosine diphosphate and monophosphate with myosin ATPase. Only carbs can be metabolized for energy without oxygen. Enzymes of the phosphagen system are myosin ATPase and creatine kinase which catalyses the synthesis of ATP from creatine phosphate and ADP. Glycolysis breaks down glucose or muscle glycogen to ATP by enzymes located in sarcoplasm. In fast glycolysis pyruvate is converted to lactic acid faster than with slow glycolysis, in which pyruvate is transported to mitochondria, sometimes giving it the name aerobic glycolysis.
Glucose+2P+2ADP yields 2lactate+2ATP+H20
Slow glycolysis: glucose +2P+2ADP+2NAD
Yields 2pyruvate+2ATP+2NADH
NADH is nicotinamide adenine dinucleotide
Simply put, glycolysis produces two molecules of ATP from one molecule of glucose, unless glycogen is used, which produces 3 ATP in phosphorylation.
The rate-limiting step is the slowest reaction in the series, which is the conversion of fructose-6-phosphate to fructose-1,6 bi-phosphate by phosphofructokinase. Glycolysis is stimulated by ADP, P, ammonia, slight decrease in pH and AMP. It is inhibited by lowered pH, inadequate oxygen supply, increased levels of ATP creatine phosphate, citrate, and free fatty acids. As lactic acid accumulates, there are more H ions which can inhibit glycolysis, maybe the calcium binding to troponin or the actin-myosin cross-bridge formation. Lactic acid is converted to its salt lactate by buffering systems in muscle and blood, but lactate doesn't cause fatigue, as it is an energy substrate used for Type I and cardiac muscles and gluconeogenesis, the formation of glucose from non-carbs. Actually blood lactate concentrations reflect lactic acid production and clearance. The Cori cycle occurs when lactate is transported in the blood to the liver. Normal concentration of lactate at rest is 0.5 to 2.2. Peak blood lactate concentrations occur five minutes after the cessation of exercise. The lactate threshold begins at 50% to 60% of maximal oxygen uptake in untrained subjects and at 70% to 80% in trained subjects. OBLA, or the second onset occurs when the concentration is near 4mmol l.
Oxidative system metabolizes carbs and fatty acids as substrates, only protein after 90 minutes or during starvation. Then it (usually branched chain amino acids) may contribute 3% to 18% of energy requirements. Urea and (toxic) ammonia are by-products. At rest approximately 70% of ATP is derived from fats 30% from carbs. High intensity almost 100% from carbs. If there is enough 02 then pyruvate is not converted to lactic acid but transported to mitochondria and converted to acetyl CoA and then enter the Krebs cycle for further ATP production, along with two NADH molecules produced during glycolytic reactions. The Krebs cycle produces two ATPs indirectly from guaninetriphosphate for each molecule of glucose, and six molecules of NADH from one molecule of glucose and two molecules of reduced flavin adenine dinucleotide or FADH2. These molecules transport hydrogen atoms to the ETC. ETC (Electron Transport Chain) uses NADH and FADH2 to rephosphorylate ADP to ATP. One molecule of NADH can produce three molecules of ATP, whereas one molecule of FADH2 can produce only two molecules of ATP�oxidative phosphorylation. Oxidative system produces 38 ATPs from one molecule of glucose. The rate-limiting step in the Krebs cycle is the conversion of isocitrate to a-ketoglutarate, a reaction catalyzed by the enzyme isocitrate dehydrogenase, which is stimulated by ADP, and inhibited by ATP.
Fats are broken down: Triglycerides stored in fat cells broken down by lipase, which releases free fatty acids into the blood, where they can circulate and enter muscle fibers, and undergo meta oxidation in the mitochondria, resulting in the formation of acetyl CoA and hydrogen atoms. The acetyl CoA enters the Krebs cycle, and the hydrogen atoms are carried by NADH and FADH2 to the ETC.
All 3 systems work together but one predominates, based on intensity and duration, from 5 seconds to an all day marathon.
0-6sec: Very intense, Phosphagen, Rate of ATP (1), Capacity (5)
6-30sec: Intense, Phosphagen and Fast Glycolysis, Rate of ATP
30sec to 2 min: Heavy, Fast Glycolysis, Rate of ATP (2), Capacity (4)
2-3 min: Moderate, Slow Glycolysis, Rate of ATP (3), Capacity (3)
>3min: Light/Moderate, Oxidation of carbs, Rate of ATP (4), Capacity (2)
Longer duration aerobic activity: Light, Oxidation of fats and proteins, Rate of ATP (5), Capacity (1)
Anaerobic contribution to exercise is oxygen deficit; post-exercise oxygen uptake is oxygen debt of EPOC.
BIOMECHANICS
Torque is the magnitude of the force multiplied by the length of its moment arm. A mechanical advantage greater than 1.0 means that the force exerted on the resisting object by the lever is greater than the applied force, as in a second class lever (rising on your toes). When the mechanical advantage is less than 1.0, as in a third class lever (most synovial joint actions), the lever exerts a smaller force on the resisting object than the force applied to the lever.
First class lever (seesaw, atlanto-occipital joint) �applied and resistive forces on opposite sides of the fulcrum.
Work = Force times Distance
Power = Force times Distance divided by Time
Work = weight x vertical distance x reps (weight lifting)
Angled sleds: actual resistance =sine of the floor-to-track angle x weight of the sled plus added plates
SI is French for systeme internationale.
Pounds x 4.448= newtons
Newtons x 0.2248= pounds
Kilograms force x 2.205= pounds
Pounds x 0.4536= kilograms force
Kilograms force x 9.807= newtons
Newtons x 0.1020= kilograms force
Feet x 0.3048=meters
Inches x 0.02540=meters
Miles x 1,609= meters
Foot-pounds x 1,356=joules
Foot-pounds per second x 1.356= watts
Horsepower x 745.7=watts
Miles per hour x 1,467=feet per second
Miles per hour x 0.4470=meters per second
Degrees x 0.01745= radians
Energy efficiency of muscular activity is in the 20% to 30% range, so energy consumed is about four times the mechanical work produced. A person who can maintain a power output of 200 watts for several minutes while running or cycling may be able to average 1,500 watts during a vertical jump.
The strength-to-mass ratio equals the force the person can exert during a particular movement divided by the mass of the body.
Resistance during exercise: gravity, inertia, friction, fluid resistance, and elasticity.
The force of attraction between any two objects is proportional to the product of the objects' masses and inversely proportional to the square of the distance between them.
An object has the same mass wherever it is, but its weight is the object's mass times the local acceleration due to gravity. Since the pound is a unit of force, it cannot correctly be applied to a weight plate. Better to say, �He lifted 10 kilos.� The moment arm of a weight is always horizontal because it produces a torque perpendicular to the line of action of the force. The torque about a given body joint when a weight is held is the product of the weight and the horizontal distance from the weight to that body joint. Therefore the lifter must exert the greatest muscular torque to lift the barbell in a biceps curl when the forearm is horizontal. In a squat, greater forward trunk inclination positions the weight horizontally farther from the hip, increasing the resistive torque about the hip, making hip extensors work harder. When the bar is low on the back, trunk must be inclined forward, making hip extensors work harder, knee extensors less. When the bar is high, there is less trunk inclination and more work is shifted to knee extensors. Front squat requires less forward lean so that greatest possible load is on quads. To mitigate stress on back the feet can be positioned a foot or 30 centimeters forward of their normal position on the Smith, making the trunk stay more upright, decreasing the horizontal moment arm about the lower back, reducing the torque the back muscles must generate, making quads work harder because the length of the horizontal moment arm about the knee is increased.
Machines can have levers, gears, cams, pulleys, cables, pressure so you can't determine the force unless you weight the plates and analyze the leverage system.
In cam-based weight-resisted machines, the moment arm through which the weight acts (horizontal distance from chain to pivot point) varies during the exercise movement. When the cam is rotated from position 1 to position 2, the moment arm of the weight, and thus the resistive torque, increase.
A client's body weight is roughly proportional to body volume, ( a cubic measure) while the ability to provide oxygen to working muscles is dependent on the cross-sectional area (a square measure) of the blood vessels, so as body size increases, there is a reduced maximal rate at which oxygen can be supplied to working muscles. A smaller fit client may have better VO2 max than a larger one, given the same variables.
Buoyant force pushing up on the body is equal to the weight of the water displaced by the body.
Inertia is the resistance to acceleration, and acceleration is the change in velocity divided by the change in time. Force equals mass times acceleration. Only when a mass is supported in a static position or lifted and lowered at a constant rate is the resistive force equal to the force of gravity on the mass, and the direction of the resistance is only downward. However, if there is any acceleration at all, it is accompanied by inertial resistance in addition to gravitational resistance. Inertia equals mass times acceleration, and the direction of the inertial resistance is opposite to the direction of the acceleration.
If the upward force on a bar drops to zero, the bar is in free fall, with its downward velocity increasing every second by 32 feet 9.8 meters per second. If the lifter desires to slow the downward velocity of the bar, then the lifter must exert upward force on the bar that is greater than the bar weight. If the lifter waits until the bar is close to its low point before slowing down its descent, and the bar must be brought to a stop in a very short time, the force of deceleration can greatly exceed bar weight and cause injury. During a power clean with a heavy weight, the strong leg, hip, and back muscles accelerate the bar vertically to a high enough velocity that even though the weaker upper body muscles cannot exert vertical force equal to the bar's weight, the bar continues to travel upward until the force of gravity decelerates the bar to zero velocity at the top of the lift. More work against gravity per unit time is done in the body at a faster cadence and more work against inertia is performed per unit time due to faster cadence and forces of acceleration.
Bracketing is a type of training with lighter- and heavier- than normal resistance training speed and strength.
When two substances rub together they create friction. Belt- or brake pad-resisted cycle ergometers and frictional wrist curl devices use this principle. The resistive force is roughly proportional to the force pressing the two surfaces together, and it takes more force to get it started than to keep it moving. Once the movement starts, the resistance does not change much even as speed changes. The Slide uses friction, as the work of the push-off leg depends on the weight of the client, the level of friction between the board and booties, and the distance between the ends of the board. A cord passed through a raking device provides concentric resistance.
Fluid resistance is used in swimming, skydiving, javelin throwing etc, although properties of water differ from air. In hydraulic machines, the fluid is a liquid, while in pneumatic machines it is a gas. Fluid resistance comes from surface drag, caused by the friction of fluid molecules passing along the surface of an object, and form drag, caused by the force of the molecules pressing against the front or rear of an object passing through the fluid. Swimmers try to minimize form drag by offering the least amount of cross-sectional area in the direction of travel. The angle of attack is the angle of the swimmer's body relative to the horizontal, smaller angle, less drag. Turbulence of water can work for or against movement. The longer the swimming race, the more fat can help create buoyancy and insulate against cold. Aqua aerobics seeks to increase drag, friction, and use buoyancy to increase resistance and intensity. In water up to the neck, client supports only 10% of body weight, whereas at waist level, she must support 50%.
Fluid-resisted machines are controlled by velocity of piston movement; cylinders allow rapid acceleration early and less when high speeds are reached. The increasing resistance with increasing speed limits the rapidity of the movement. Usually this is concentric, unless specifically designed with pumps. Most fluid resisted exercise is concentric/concentric unless special apparatus thwarts this tendency.
Boats must also be streamlined for speed or chunky for strength.
With elastic band resistance, the tension increases with the degree of stretching, beginning with low, ending with high resistance to hold the position statically, the opposite of most free weight exercises.
PTs use isokinetic dynamometers to maintain constant joint angular velocity by matching resistive force to muscle force with variable resistance.
Gravitational potential energy is the product of the object's weight and the distance it can fall, while kinetic energy is one-half the product of the object's mass and the square of its velocity. The amount of negative work performed in decelerating a moving object to zero velocity is equal in magnitude to the object's kinetic energy before it is decelerated. The total negative work is the sum of the work of lowering and of decelerating. Because power equal work divided by time, negative work results in negative power. ACL tears from sudden stops or changes in direction.
Adaptations to Resistance Training:
For the first 8-12 weeks, hypertrophy of muscle fibers is usually not measurable but neurological adaptations in terms of EMG amplitude, number of motor units etc have increased, along with changes in myosin heavy chains and myosin ATPase to allow for more rapid and forceful contractions.
Acute changes:
EMG amplitude and number of motor units recruited increase.
Hydrogen ion concentration, inorganic phosphate concentration and ammonia levels increase.
No change of slight decrease in ATP.
CP and glycogen decrease from work performed.
Epinephrine, cortisol, testosterone, and growth hormone increase.
Growth hormone and insulin are protein/peptide hormones, while testosterone and estrogen are steroid hormones derived from cholesterol, one reason that a diet of less than 15% fat will often deplete anabolic hormones. Testosterone, insulin, and growth hormone are anabolic, while cortisol is catabolic, but is essential to maintaining blood glucose levels. Epinephrine increases fat and CHO breakdown so that more ATP is available, as well as aiding CNS with motor unit recruitment.
Rate coding is the number of action potentials per unit of time; normally the faster the firing rather, the more force produced. However small muscles like hands achieve full recruitment at a low force output, while large muscles have higher recruitment and lower firing rates like the quads, making the size of the EMG signal get larger during a set of resistance training exercises to reflect changes in motor recruitment and firing rate.
The size principle dictates that motor units that innervate slow-twitch fibers innervate fewer fibers than units that innervate fast-twitch fibers, although the smaller neuron size results in a lower threshold for activation. Fast-twitch fibers are recruited even during slow contractions if the force demands are high enough.
Chronic Adaptations:
Muscle strength, power, and endurance increase, at different rates depending on focus of training.
Phosphagen system and glycolytic enzyme concentrations and/or absolute levels increase.
ATP and CP absolute levels increase, due in part to increased size. but ATP and CP changes during exercise decrease as well as lactate.
Type I CSA, Type II CSA(cross-sectional area, i.e. hypertrophy, not hyperplasia) and Type IIa increase, Type IIb decrease, Type I remains the same.
Fat usually decreases, while fat-free mass and metabolic rate increase.
EMG and motor unit recruitment and firing probably increase, while co-contraction decreases.
Connective tissue strength and bone density mass usually increase.
Resistance training does not increase VO2max but is a good adjunct to get better results from cardiorespiratory endurance.
Sarcopenia is loss of muscle mass, which occurs naturally after 30 unless mitigated by weight training.
Isometric strength detrains quickly as does anaerobic metabolic tests like the Wingate.
Aerobic Adaptations:
VO2max, aVO2 difference, stroke volume, (because of changes in pre-load, afterload and myocardial contractility), cardiac output, and oxidative capacity of muscle usually go up, but resting heart rate and submaximal exercise heart rate usually go down. The Frank-Starling effect is the stretch-reflex of the left ventricular that results in greater force. Cardiac output can be as much as four times during maximal aerobic exercise in an untrained person, six times in a male marathoner. Size of chambers increase about 40% in general with aerobics, and the ventricular wall thickens. Blood volume, plasma and hemoglobin go up, leading to greater stroke volume at rest. Maximal heart rate is not affected by training, just submaximal. There is an increase in density of capillary beds, to allow for better diffusion of oxygen and metabolites, permitting better oxygen uptake.
Acute adaptations are not that marked; chronic adaptations permit body to store more fuel, and then to utilize it through enzymatic processes at the cellular level.
Enzymes increase:
Hexokinase�responsible for phosphorylation of glucose after entry in to the cell
Phosphofructokinase�rate-limiting enzyme of glycolysis
Lactate dehydrogenase�responsible for reversible conversion of pyruvate to lactate
Succinate dehydrogenase and Citrate synthase also improve
GLUT4 increases
Mitochondria get denser.
Pancreas, (production and release of insulin and glucagon for uptake or release of glucose). Acute==increases insulin-stimulated whole-body glucose uptake for 48 hours postexercise. Increase in insulin sensitivity.
Adrenal cortex (cortisol) maintains blood sugar levels, stimulates protein conversion, utilization of fats.
Adrenal medulla has a sympathoadrenal response to exercise releasing catecholamines, epinephrine and norephinephrine, also a sympathetic nervous system response. These eventually decrease as the body becomes more efficient at exercise, reducing stress.
Studies show increase in bone mineral density site-specific at point of impact�tibia, femoral neck etc. Wolff's Law states that bone will be laid down where needed. Therefore high-impact weight-bearing activity is the most beneficial for increasing bone mineral density and the health of articular cartilage is not jeopardized during running, aerobic dance et. Adaptations occur to new stresses, then plateau.
Pulmonary ventilation obviously increases with exercise, but chronically, lung volumes, carrying capacity of blood and diffusion ability improve.
VO2max peaks naturally between 12-15 in girls, 17-21 in boys, but five middle aged men recovered 100% of age-related decline in power over 30 years after six months of aerobic training.
Overreaching is the precursor or plateau before the decline that occurs in overtraining.
NUTRITION:
Dietary intake data can be obtained from dietary recall (24 hours), history (interview), or records (3 days.)
Memorize food pyramid�fats, oils, sweets sparingly, milk, yogurt, cheese 2-3 servings, protein 2-3, vegetables 3-5, fruit 2-3, and bread, cereal, 6-11.
A serving is not a helping. Memorize:
Bread: one slice, or one dinner roll
Cereal: 1 ounce or ½ cup cooked cereal
Pasta and rice: ½ cup cooked
Raw leafy veggies: 1 cup
Other veggies: ½ cup
Fruit: one fruit
Juice: ¾ cup
Milk and yogurt: 1 cup
Cheese: 1/1/2 to 2 ounces
Meat: 2 or 3 ounces cooked (this is nothing!)
½ cup beans, one egg, 2 tablespoons peanut butter
RMR or resting metabolic rate accounts for 60% to 70% of daily energy, measure of calories needed for metabolic activities. RMR is INCREASED by lean body tissue, young age, growth, abnormal body temperature, menstrual cycle, hyperthyroidism etc. RMR is DECREASED by low caloric intake, loss of lean tissue, hypothyroidism. 20% variation due to genetic differences.
Thermal effect of food is 7% to 10% of total energy requirement. Steve weighs 77 kilos, and is so active he needs 3,900 kcal a day. Or calculate Resting Energy Expernditure, then multiply it by a factor based on activity level.
RDA for protein is .8 grams per kilo for men and women, but aerobic endurance athletes can reach 1.4 grams per kilo, and resistance training may require 1.2 to 2.0 grams per kilo, unless you have bad kidneys, low calcium, restricted fluid etc.
50-100 grams of CHO prevents ketosis from incomplete breakdown of fatty acids. Physically active people should consumer 60-70% CHO. Endurance athletes need 8-10 grams per kilo or 600 to 750 grams or 2400 to 300 kcal from CHO per day for a person weighing 165. This will restore skeletal glycogen within 24 hours. For strength, sprint, and skill 5 to 6 grams per kilo per day is reasonable. (Fruits and veggies are carbs.)
Fat: 3% from Omega 6, .5 to 1% from Omega 3. Less than 10% fat can make blood lipid levels worse; less than 15% can decrease testosterone. Women of reproductive age need at least 20% fat. Recommendations are 30% fat for average people, 35% for athletes. 9kilocal�protein and CHO 4Kilocal.
RDA is the population mean plus two standard deviations, not the minimum number.
Water requirements change according environment, sweating, body surface area, caloric intake, body size, lean muscle tissue, activity level, etc.
At least 1 pint two hours before exercise.
During and after exercise replenish fluids completely.
Muscle tissue is 70% water, 22% protein, 8% fatty acids and glycogen. 2500 extra kilocal are required for each 1 pound increase in lean tissue. 350 to 700 kilocal above normal are needed to support a 1 to 2 pound weekly gain in lean tissue as well as energy requirements of training.
An average of 1 to 2 pounds a week represents a daily caloric deficit of 500 to 1000 kcal.
DON'T recommend supplements, aids, crash diets, herbs etc, or exclude food groups such as protein, dairy, bread. Follow guidelines strictly and if there is any medical problem, refer to nutritionist.
Excess iron can lead to hemochromotasis, excess zinc can increase HDL, and excess calcium risk kidney stones. Healthy protein shakes with yogurt, fruit, flax seed etc are okay. That is it. Many liability suits come from trainers acting as nutritionists recommending specific things without a sufficient biochemical work-up.
PSYCHOLOGY
Exercise relieves trait and state anxiety, except when coupled with potential of injury in martial arts or failure in team sports.
Stress can be measured by muscle tension, blood pressure, brain electrical activity. With rhythmic aerobic exercise it is possible that cerebral cortical arousal is inhibited, due to a volley of afferent rhythmic impulses from the skeletal muscles to a relaxation site in the brain stem of the CNS. Also hypothalamus detects elevation in body's temperature and promotes cortical relaxation effect, resulting in reduced muscle tension. Release of beta-endorphins, increased serotonin and catecholamines also help to alleviate depression and reduce anxiety. This neurotrophic effect, working with oxygenation, helps preserve mental functioning.
Older men who were physically fit performed as well as young men on complex battery of cognitive challenges and better than their sedentary counterparts. Fluid intelligence (problem solving) in the frontal lobe executive processes is more affected by exercise than crystallized intelligence, which is the ability to accumulate knowledge and recognize words and recall facts.
Apolipoprotein e4 allele (APOE4) is the gene known to increase risk for cognitive impairment in the elderly.
Mens sana in corpore sano
Goal setting�SMART
Short and long term
Challenging�50% chance of success
Behavioral reinforcement
Self-efficacy
Process goals�control
Outcome goals�little control
Performance goals�in between
Task-involved, ego-involved, other-involved
Goals should be specific, measurable, observable, with time constraints, moderately difficult, but attainable, compatible, and prioritized. Record goals and monitor progress. Diversify process, performance, and outcomes. Set short-range goals to achieve long-range goals. Make sure goals are internalized.
Constructs are personality, ambition, and assertiveness, things we can't see but must imagine and infer.
Motivation includes the directional aspect that influences choices, and the intensity of pursuit of those choices.
Revisit BF Skinner, the outmoded operant conditioning man of behaviorism, with his target behavior, the operant, the reinforcement, the punishment. People have intrinsic or extrinsic motivation. Memorize following chart:
Memorize transtheoretical model for stage of readiness
Bandura's self-efficacy is a person's confidence in his/her own ability to perform specific actions leading to a successful behavioral outcome, influenced by performance accomplishments, modeling effects, verbal persuasion, and physiological arousal or anxiety.
a. Minimize procrastination
b. Identify false beliefs
c. Identify and modify self talk changing negativity to affirmations
d. Mental imagery including Jacobsen's progressive relaxation
e. Visualization from past, future, present states�ideokinesis�yeah!
Let the past go.
Do your best; don't be perfect.
Express yourself and keep track in a journal.
Go from familiar to unfamiliar.
Offer choices.
Provide feedback.
Use social support systems.
Have client create positive affirmation.
CLIENT CONSULTATION AND HEALTH APPRAISAL
Motivate, assess, train, educate, and refer.
Follow these exact steps:
7CAD risk factors: a. family history: if a myocardial infarction, coronary revascularization, or sudden death occurred before 55 years of age in father or first-degree male relative, or before 65 in mother or first-degree female relative.
b. cigarette smoking
c. hypertension (over 140-90) because of increased wall stress, which increases the workload of the heart in pumping the extra blood required to overcome peripheral vascular resistance.
d. hypercholesterolemia�LDL>130mg/dL or on lipid-lowering medication. Over 60 HDL is a negative CAD factor because some doctors use combined cholesterol over 200 as a cut-off.
e. impaired fasting glucose levels over 110mg/dL, confirmed on 2 occasions. Diabetes mellitus, a metabolic disease, is characterized by hyperglycemia resulting from defects in insulin secretion in type I, insulin action in type II, or both. Diabetes increases risk for CAD, peripheral vascular disease, and congestive heart failure.
f. obesity�BMI =or>30, which is 30 kilograms bodyweight per height in meters squared or a waist girth 39 inches or 100 cm.
g. Sedentary lifestyle is defined as people who do not participate in a regular exercise program or meet the minimal physical activity recommendations of 30 minutes or more of accumulated moderate-intensity activity on most, or all days of the week to expend approximately 200 to 250 calories a day.
In addition to interpreting questionnaires, PTs must evaluate signs and symptoms of cardiovascular and pulmonary disease:
COPD
Asthma: spasmodic contraction of smooth muscle around the bronchi that produces swelling of the mucosal cells and an excessive secretion of mucous that constricts airway paths caused by allergic reactions, exercise, air quality factors, and stress.
Chronic bronchitis: an inflammatory condition caused by persistent production of sputum due to a thickened bronchial wall, which in turn creates a reduction of airflow.
Emphysema: an enlargement of air spaces accompanied by the progressive destruction of alveolar-capillary units leading el elevated pulmonary vascular resistance, and perhaps heart failure.
INITIAL RISK STRATIFICATION uses age, health status, personal symptoms, and coronary risk factors to classify individuals into one of three risk categories for preliminary decision-making purposes.
PAR-Q
Memorize: a. Has your doctor ever said that you have a heart condition and that you should only do physical activity recommended by a doctor?
b. Do you feel pain in your chest when you do physical activity?
c. In the past month, have you had chest pain when you were not doing physical activity?
d. Do you lose your balance because of dizziness or do you every lose consciousness?
e. Do you have a bone or joint problem that could be made worse by exercise?
f. Is your doctor currently prescribing drugs for blood pressure or heart?
g. Do you know of any other reason you should not do physical activity/
One yes�and go to the doctor for clearance.
Health/Medical questionnaires evaluates complete medical history, family history, activity history, medications, goals.
From the initial risk stratification�refer moderate risk individuals to physicians for vigorous exercise (over 6 METS or greater than 60% maximal oxygen uptake) or maximal testing, and high risk individuals for everything. Moderate exercise is 3-6 METS, and submaximal tests are field tests performed by PTs.
If a client gives YES to one or more questions on the PAR-Q, refer to a physician. Pregnant�get clearance, as well.
TESTING
Base-line Data
Evaluate
Formative evaluations include formal assessment with a specified test protocol, and subjective observations such as posture, comments, body language etc.
Compare performance with norm-referenced standards in percentile values against other individuals in a like category, and criterion-referenced standards show whether a health standard was met.
Summative evaluations represent the sum total of what the client did during a training period, class, or season.
Assessment is the act of measuring a specific component using a well-constructed, valid, (i.e., relevant and truthful, in terms of content, construct and criterion-related validity), and reliable (repeatable) test with calibrated equipment, with a well-prepared subject, and accurate, meticulous protocol and planning, given a standard error of measurement.
If a client is sedentary, over 60, or has a functional aerobic capacity of five METS, or is a preadolescent, the YMCA Step test, or 1.5 mile (2.4 kilometer) or 12 minute run aren't appropriate. The bike or a one-mile walk test might be better.1RM testing (squats and bench press) may be bad for untrained, overweight, arthritic individuals, so that 10RM testing would be necessary.
Aerobic testing is impaired with temperatures over 80 degrees F or 27 C when humidity exceeds 50%, or less than 25 degrees F or -4C. It can take 10 days to acclimate to altitude even 1,900 feet or 580 meters. Indoors, room should be 68-72, 60% or less humidity, and air circulation of 6 to 8 exchanges per hour.
Indications for Stopping an Exercise Test in Low-Risk Adults
Angina
Significant 20mmHg drop in systolic blood pressure, or failure of blood pressure to rise
Excessive rise in blood pressure >260/115
Light-headed, confused, ataxia, pallor, cyanosis, nausea, or cold, clammy skin
Noticeable change in heart rhythm
Client requests to stop
Severe fatigue
Failure of testing equipment
Client must get adequate sleep the night before and no vigorous exercise 24 hours before test
Light meal or snack 2-4 hours before
6-8 glasses of water day before test and at least two cups of water in two hours prior to test
Abstinence from chemicals
Proper attire
Knowledge of procedures and expectations
Conditions for terminating test
NSCA has a different test sequence than ACSM
General Fitness
Athletes
1. Resting tests of HR, BP, height, weight, and body composition
If possible, perform maximal aerobic tests on a separate day, or wait after an hour rest.
If client scores below average, begin 2-3 times a week at moderate intensity, and work up.
Heart Rate (brachial, carotid, radial, or temporal)
Stopwatch
Stethoscope� Bell should be placed directly on the skin over the third intercostal space just left of the sternum for 30-60 seconds.
Heart Rate Monitor
Shorter-duration during exercise�6, 10, or 15; 30-60 for resting
Blood Pressure
Listen for Korotkoff sounds with a mercury or aneroid sphygmomanometry�need an inflatable air bladder, and a stethoscope (cuff or auscultatory method)
1.No smoking or caffeine 30 minutes before
2.Sit upright in a chair with back support, either arm exposed, supinated, and supported, at level of heart.
3.Select appropriate cuff size by taking arm circumference measurements midway between the acromion process of the scapula and the olecranon process of the ulna.
4.Rest for a minimum of five minutes.
5.Place the cuff on the arm so that the air bladder is directly over the brachial artery and the bottom edge of the cuff is one inch or 2.5cm above the antecubital space. With the client's palm facing up, place the stethoscope firmly, but not hard enough to indent the skin, over the antecubital space. Use dominant hand to control the bladder airflow by placing the air bulb in the palm and using the thumb and forefinger to control the pressure release. The nondominant hand is then used to hold the stethoscope.
6.Position the sphygmomanometer so that the center of the mercury or aneroid dial is at eye level and the air bladder tubing is not overlapping, obstructing, or being allowed to freely contact the stethoscope head or tubing.
7. Once the cuff, the stethoscope, and the sphygmomanometer are in place, quickly inflate the air bladder to 160mmHg or 20 mmHg above anticipated systolic reading. Upon maximum inflation, turn the air release screw counterclockwise to release pressure at 2-3 mmHg per second.
8.The first audible detection of Korotkoff sounds is SBP, and the last audible detection of Korotkoff sounds is DBP. These sounds are similar to extraneous noises made when the air bladder tubing is allowed to bump against the stethoscope bell so avoid this.
9. Observe manometer for an addition 10 to 20 mmHg of deflation to confirm absence of sounds, then release the remaining pressure, and remove cuff.
10. After a minimum of 2 minutes rest, measure BP again using the same technique. If they differ by more than 5mmHg, take a third reading. Average the scores.
Check to see if stethoscope is on backward, if the stethoscope bell is under the cuff, if the dial is not at the tester's eye level, or if the blood pressure cuff is positioned too close to the antecubital space.
Body Mass is weight in kilos divided by height in meters squared.
Measure height with feet together, shoes removed, breath held, and then convert inches to centimeters. Convert the weight in pounds to kilos. Pounds divided by 2.2046=kilos. Consult chart for BMI.
Skin-fold Measurement
Errors can be compounded by
BIA is Bioelectrical Impedance�not as accurate for very lean or obese
NIR is near-infrared interactance
Waist-to-Hip Ratio with a plastic or metal tape measure
Divide waist by hip circumference and consult chart. These range from <0.83 to >0.94
Cardiovascular submaximal testing
Cycle ergometer
The YMCA Cycle Ergometer Test is a submaximal, multistage exercise test for cardiovascular endurance, set at 50RPM, designed to progress client to 85% of predicted maximal HR using three-minute stages of increasing work rate. The following data is needed to plot the heart rate with charts, graphs, and equations:
Body weight in kilograms, age-predicted maximal HR, at least two measurements at each work rate up to 85% of age-predicted maximal HR, a BP measurement at each work rate, an RPE assessment at each work rate
The Astrand-Rhyming Cycle Ergomenter Test is a single-stage test lasting six minutes with cadence at 50RPM, from >61 to <13.
The YMCA Step Test
12-inch step at 96BPM for 3 minutes, 24 steps per minute, Up, Up, Down, Down
Within 5 seconds, measure heart rate for three minutes
Compare this to normative values�70- 151�excellent to poor.
Distance Run and Walk tests
Running a greater distance in less time is a way to assess cardiovascular endurance in healthy men under 40 and healthy women under 50.
12 minutes, 1 mile or 1.5 miles
12 min: 400-meter (437 yard) track or flat course with measured distances so that the number of laps completed can be easily counted and multiplied by the course distance.
Record the total distance in meters. (400 meters times 5.25 laps = 2,100 meters.)
VO2Max=[0.0268 times (D)]-11.3
Then compare to estimated norms in chart.
1.5 mile run is also a field test used in a regressive equation to estimate VO2max,
but the score is converted to minutes by dividing by 60 and then using this equation: VO2max=88.02-(0.1656 times BW) �(2.76 times (time) + (3.716 times gender) For gender, substitute 1 for males, and 0 for females.
Rockport Walking Test is good for everyone 18-69. After walking a mile as briskly as possible, use a 15-second duration to count HR, then convert the seconds to minutes by dividing by 60. Estimate VO2Max with another long equation. <10-12 to <17.32 excellent to poor.
Muscular Strength
1RM Bench Press requires skill because a barbell is used.
• Warm-up with a light weight for 5-10 reps.
• 1 minute rest.
• Estimate load for 3-5 reps increasing 5-10% for upper body, 10-20% for lower body.
• 2 minute rest.
• Estimate a conservative, near max load for2-3 reps, increasing 5-10% for upper body, 10-20% for lower body.
• 2-4 minute rest.
• Load increase 5-10% for upper body, 10-20% for lower body for 1 RM.
• 2-4 minute rest.
• Increase load and try again if client was successful. Decrease 2.5% for upper body or 5-10% for lower body if client failed.
• Divide the 1RM value by the client's body weight to determine relative strength and then compare to normative chart�1.48 to 0.53 in men, 0.54 to 0.02 in women.
1RM needs a Universal leg press machine for the normative data, but you could use an angled hip sled or horizontal leg press.
Standardize knee angle at approximately 120 degrees. Norms�2.27 to 1.16 for men, 2.05 to 0.75 for women.
Muscular Endurance
YMCA Bench Press: Set resistance at 80 pounds (36.3kg) for men, 35 pounds (15.9kg) for women. Set metronome at 60BPM for a rate of 30 reps per minute. Have the client, beginning with arms extended and a shoulder-width grip, lower the weight to the chest. Then, without pausing, the client should raise the bar to full arm's length. The bar should reach the highest and lowest positions with each beat of the metronome. Terminate when the client can no longer lift. Norms are 44 to 0
Partial Curl-Up
• Lie supine with the knees at 90 degrees. Arms are at the side on the floor with the fingers touch a four-inch (10-cm) piece of masking tape that is placed on the floor perpendicular to the fingers. A second piece of masking tape is placed 8 cm or 3 inches (for those who are under 45) and 12 cm or 5 inches for those who are over 45).
• Set a metronome to 40BPM and have the individual do slow, controlled curl-ups to lift he shoulder blades off the mat (trunk makes a 30 degree angle with the mat) at 20 curl-ups per minute.
• Perform as many curl-ups as possible without pausing, up to 75.
Norms are 75 to 0.
One Minute Sit-Up
• Lie supine with arms crossed on chest, hands touching shoulders, heels approximately 12-18 inches (30-45 cm) from the buttocks.
• Using a stop watch for 60 seconds have client raise torso until it is perpendicular to the floor. The chin should be tucked into the chest, and the hands should stay in contact with the shoulders. The client then lowers the torso until the shoulders are once again in contact with the floor. Rest periods are allowed.
• Compare score to norms�77-8.
Push-Up Test
This test becomes one for muscular strength rather than endurance when the body weight is too heavy to complete multiple reps.
• Assume push-up position. For men, the hands are shoulder-width apart, the back is straight, and the head is up. Women can flex the knees to 90 degrees and cross the ankles.
• For a male client, place a fist on the floor beneath his chest, counting the reps only when the chest touches the fist. For female clients, you can use a foam roller and then raise body to full arm's length.
• Record number of reps and compare to norms�41 to 2 for men, 31 to 0 for women.
Sit and Reach
There is no test to measure whole body flexibility. Sit and reach can measure hip and back flexibility, but, because of many variables such as torso-leg length ratio etc., it is not always 100% accurate.
• Warm-up and take off shoes.
• For YMCA test, place a yardstick on the floor and place tape across the yardstick at a right angle to the 15-inch (38cm) mark. The client then sits with the yardstick between the legs, extending the legs at right angles to the taped line on the floor. The heels should touch the edge of the taped line and should be about 10-12 (25-30cm) apart.
• When using a box, place the heels against the edge of the box.
• Have the client reach forward slowly with both hands, moving as far as possible and holding the terminal position. The fingers should overlap and be in contact with the yardstick or the sit and reach box.
• The score is the most distant point reached. Use the best of three scores. The knees must stay extended, but the trainer should not press the knees down. Norms are 22-4 for tape, 42-11 for sit and reach box. Women score better on this test, finally!
Memorize high and low percentile values for common tests
VO2max Men 20-29 51.4
Women over sixty 20.8
So if a 39 year old woman's Vo2 max is 30.2ml kg min she needs to work on aerobics.
Muscles are elastic, tendons and ligaments can be elastic and plastic. Warm-ups can be passive, general, or specific, stretching ballistic, static, dynamic, or PNF. NSCA PNF technique is a 10 second passive stretch, followed by a 6 second isometric contraction against partner resistance, followed by a 1-2 second rest, and another 30 second passive stretch followed by a deeper stretch. Since usable, functional strength is crucial, dynamic stretches such as arm circles, arm swings, and hockey lunges are important.
Ant.deltoids and Pecs : Hands behind back
Triceps and lats: Behind-neck stretch
Obliques, piriformis, ITB, erector spinae: Pretzel
Iliopsoas, glutes, quads, hams: Lunge
Glutes, hams, back: Knee to chest, walking knee tuck
Back, hams, gastroc: Semistraddle
Adductors, Butterfly, Knee over hurdle
Calves: Wall stretch
NSCA supports back extension and rotation lying prone.
Hands crossed over chest for curl-ups or squat chair test.
All stability ball exercises in every position including advanced pikes are okay for core.
Grips are pronated, supinated, alternated,
neutral, open, closed
5 point contact: Head, Shoulders, Buttocks, Right Foot, Left Foot
Pronators: straight last, high motion control
Supinators: curved last, high motion flexibility
Cardio Machines
Treadmill: Quads, hams, glutes, iliopsoas, tibialis anterior, gastroc, soleus
Stair climber: Quads, hams, glutes, iliopsoas, tibialis anterior, gastroc, soleus. Don't face out on climber. Excessive leaning can compromise posture and reduce caloric consumption up to 20%. Avoid too much lateral sway. Reduce step depth or speed until proper form is achieved. 43-95 steps per minute.
Elliptical: Quads, hams, glutes, iliopsoas, tibialis anterior, gastroc, soleus.
Don't let knees bend more than 90 degrees over toes.
Bike: Quads, hams, glutes, iliopsoas, tibialis anterior, gastroc, soleus
Less lower leg than treadmill, especially on reclining bikes. Seat height�slight bend in knee when ball of foot is at 12 o clock. Strongest push from hip extension is between 45 and 135 degrees. HR, BP, VO2 max, rate-pressure product, and RPE lower in reclining bikes because back support alleviates postural workload, and reclining position reduces need for heat to pump blood vertically against gravity.
Rowing Machines: Quads, hams, glutes, iliopsoas, tibialis anterior, gastroc, soleus, biceps, brachioradialis, brachialis, rectus abdominis, delts, traps, lats, teres major, flexor and extensor carpi ulnaris. 70% to 75% of pulling action must come from stronger leg and hip muscles. Maintain lumbar lordosis. Torso leans forward with the start and the recovery, and back with drive and finish, but if clients have bad backs, keep torso upright and still. After hips and knees are extended in the drive, the arms pull the handle to the abdomen. Cadence is 20 for recreational to 35 for elite rowers per minute.
Walking
Stride length and stride frequency
Racewalking utilizes a pelvic roll�internal rotation on the reach of the striding leg, neutral position in mid-stance, external rotation on propulsion.
For long distance, arms relax with a slight bend and swing; for racing the arms bend at the elbows to ninety degrees. 2-4 times body weight.
Avoid braking from overstriding because too much time in the air with a staccato landing is inefficient. Understriding prevents body from advancing naturally.
Increase rear leg drive by strengthening and stretching, as well as plyo.
Impact
SLOW overstride can create a harder landing and more chance of injury.
Low impact�1 to 1/1/4
Medium�2 to 21/2
High�often greater than 3 times body weight
Step�from 1.4 to 2.5 depending on step height and propulsive moves
Swimming can use every muscle in the body. Economize during entry/catch and power phases with or without S stroke. Swimming tries to decrease drag, friction, and turbulence, while aquatics to increase them by creating moves that make it difficult (walking, jogging, kicking, jumping, and scissors in different directions and different speeds) and using resistive equipment. A body submerged to the waist bears 50% of its weight, to the chest 25%-35%, and to the neck 10%. LSD, pace/tempo, interval, repetition, and Fartlek time intervals as well as DWR can be used in the water for cross-training, rehab etc.
Initial consultation and assessment
Choice
Frequency
Order
Load
Volume
Rest
Variation
Progression
BEGINNER: 1-2 months. 1-2 times a week. Low intensity. 3-5 machine exercises. 4-6 months. 2-3 times a week. Low to medium. 6-10 machine core and assistance exercises; 3-5 free weight assistance exercises.
INTERMEDIATE: 8-10 months. 3 times a week. 11-15 machine core and assistance exercises; 6-10 free weight assistance exercises; 3-5 free weight core exercises. 1 year. Medium to high intensity. 4 times a week. 15 free weight and machine core and assistance exercises.
ADVANCED: 1-1 1/2 years. 4 times a week. High intensity. 15 free weight and machine core and assistance exercises. 3-5 power/explosive exercises.
More than 2 years: 5 times a week. Very High. 15 free weight and machine core and assistance exercises. Most power/explosive exercises.
Progression
2 for 2 rule: If a client can complete two more repetitions than the repetition goal in the final set of an exercise for two consecutive training sessions, then the trainer should increase the load in all of the sets of that exercise for the next training session.
2.5% for core, 1-2% for assistance for Beginner A, 5% for core, 2.5-5% for assistance for Beginner B
2.5-5% for Intermediate/Advanced Upper Body
5-10% for Lower Body
Core exercises involve two or more joints, and recruit one or more large muscle groups (pecs) with synergistic help of smaller groups (triceps) like the bench press. A core exercise that puts axial stress on the spine like the power clean, shoulder press, back squat is called a structural exercise. Power or explosive are structural exercises done very fast like push press, power clean, snatch, high pull. Assistance exercises are isolated, one joint exercises, even with large muscles like dumbbell fly.
Split routine�4 times a week can include light and heavy days for upper and lower body. Or 3 days on, one day off.
Potential sequences
Power, other core, then assistance
Multijoint then single joint
Large muscles then small muscles
Alternate push and pull
Alternate upper body then lower body
Core, then assistance, then alternate push/pull
Compound set is doing the same muscle�bench press, pec deck
Superset is agonist/antagonist
1RM
Limitations: Well-trained clients can sometimes exceed these limits because of neuromuscular efficiency
Applies to one set
Usually relates to power clean, back squat, and bench press�machines are easier, assistance exercises use less weight
But memorize relationships anyway:
100 1
95 2
93 3
90 4
87 5
85 6
83 7
80 8
77 9
75 10
70 11
67 12
65 15
Muscular endurance <67 >12, 2-3 sets, 30 seconds or less rest
Hypertrophy 67-85 6-12, 3-6 sets, 30-90 seconds rest
Strength >85 <6, 2-6 sets, 2-5 minutes rest
Light day is 80% of load lifted on a heavy day.
Progression
2 for 2 rule: If a client can complete two more repetitions than the repetition goal in the final set of an exercise for two consecutive training sessions, then the trainer should increase the load in all of the sets of that exercise for the next training session.
2.5% for core, 1-2% for assistance for Beginner A, 5% for core, 2.5-5% for assistance for Beginner B
2.5-5% for Intermediate/Advanced Upper Body
5-10% for Lower Body
Aerobic Training
LSD�30 minutes to 2 hours or more. 50% to 85% or HRR, Talk test.
Pace/Tempo�Exercise at their lactate threshold, RPE of 13-14 or 4-5, only one ot two times a week.
Interval Training�3-5 minutes with a rest period of 1:1 or 1:3.
Repetition�Very high intensity 90-100%, sometimes with 1:10 or longer rest periods
Fartlek�Intense bouts on an LSD base
Cross-training is good to overcome limitations of specificity and avoid injuries.
Circuit training is good when pressed for time. In general, periodization is based than combined training, although both resistance and aerobic training are necessary at different times, and even in periodization, neither program is entirely eliminated.
SEC or Series Elastic Component is composed mainly of tendons, acting as a spring, during an eccentric muscle action, storing elastic energy. If the muscle immediately begins a concentric activity, the energy is released; otherwise, it is lost in heat. Muscle spindles are intramuscular organs sensitive to the rate and magnitude of a stretch, which potentiate activity in the agonist muscle.
Resting position: Alignment and intent
Countermovement or eccentric phase: SEC undergoes a rapid stretch, muscles spindles send a signal to spinal cord
Amortization phase: Signal reaches spinal cord and synapses, signal sent back to muscle
Concentric phase: Jump up, as SEC shortens to resting length, signal reaches muscle to cause concentric action
Plyo can increase bone density up to 7%.
Children should avoid plyo because of epiphyseal plates that have not closed yet, and elderly with osteoporosis or arthritis could incur stress fractures or other problems.
In the strength training for plyo, make sure you include ECCENTRIC actions. It's not just about jumping high, but landing well, acceleration/deceleration, and changing directions efficiently and rapidly.
Needs Analysis
Age, resistance training, injury history, physical testing (vertical and standing long jump), training goals, risk of injury at job or sport
Recovery time�48-72 hours
Recovery for depth jumps may consist of 5-10 seconds of rest between reps and two to three minutes between sets.
Intensity ranges from low-level skipping to depth jumps. Beginners can do simple skips, double leg jumps-in-place, double leg standing jumps.
Volume is expressed as number of foot contacts or throws and catches, ranging from 40 to 140.
General and specific warm-ups are required. (Whole body cardio, and lower intensity rehearsal of tasks or sport.) Warm-up drills can include lunging forward, diagonal, backward, toe jogging, straight-leg jogging, butt-kickers, skipping, and footwork like sliding, shuffling, carioca, backward running or back pedaling.
STRENGTH: The client's 1RM squat should be at least 1.5 times his or her body weight. For upper body plyo clients over 220 pounds (100kilos) should have a bench press 1RM of at least 1.0 times their body weight, while those under 220 should have 1.5 times their body weight. Or perform 5 clap push-ups in a row.
SPEED: The client should be able to perform 5 reps of the squat and/or bench press with 60% body weight in five seconds or less.
BALANCE: Beginners must stand on one leg for 30 seconds without falling, intermediate a single-leg quarter squat, and advanced a single-leg half squat for 30 seconds.
SURFACE: Grass field, suspended floor, rubber mats are good but concrete, tile, and hardwood are not. Excessively thick mats or mini-trampolines may extend amortization phase, not allowing efficient stretch reflex.
Boxes must be sturdy with a non-slip top, 6-42 inches (15-107cm)
Shoes should have good ankle and arch support, lateral stability, and a wide, nonslip sole.
Speed-strength is maximum force at high velocities like power clean, hang clean, and snatch, and plyometrics. Speed-endurance is running speed and movement over six seconds.
SPRINTING: Sprinting is a series of ballistic strides where the body is repeatedly launched forward as a projectile. The body should lean forward approximately 45 degrees during acceleration and should quickly move upright to less than 5-degree lean from the ground, not the waist, during maximal speed. Put weight over ball on mid-stance, and increase height foot moves toward buttocks (heel kick). The hip then flexes with the knee around 90 degrees then becomes nearly straight as the foot moves down and forward during flight. At foot strike, hips over under and ground contact time is minimal to allow for explosive movement. Arm swing is fast and aggressive, with hands rising to nose in front and pass buttocks behind. Stride frequency is easier to train than stride length, which is more dependent on body height and leg length.
Sprint-assisted training can be done with downgrade sprinting (3-7 degrees), high-speed towing, a high-speed treadmill, a faster partner etc. This will increase the stride frequency, but don't do more than 10% of client's natural speed.
Resisted sprinting can increase client's stride length by increasing the client's ground force production during the support phase. Don't increase external resistance by more than 10%. You can use upgrade treadmill, or resistance with sled, elastic tubing, parachute, water, partner etc.
You can also sprint/walk/run with intervals.
Non-athletes could do speed 1-2 times a week, athletes 2-4 times, but not every day.
Speed recovery times: 1:5, 1:10.
Volume is expressed as distance covered.
Warm-up should be low intensity dynamic movements.
Either lower body plyo, speed training, or lower body resistance training on a given day but you can combine upper and lower body with different modalities. Complex training of plyo and resistance requires significant rest in between. A squat jump with 30% of 1RM is good for experts.
Skip: Low Horizontal and vertical.
Double-leg Tuck Jump: Medium. Vertical. Begin with a countermovement
Advanced�one-leg only
Split Squat Jump: Medium. Advanced�switch legs in the air.
Standing Long Jump: Low.
Double-leg Vertical Jump: Low. Advanced�one leg only.
Double-leg Hop: Medium. Horizontal and vertical. Advanced�one leg only.
Front Barrier Hop: Medium. Horizontal and vertical. Advanced�increase height of barrier.
Alternate Leg Bound with double arms. Medium, Horizontal and vertical.
Jump to Box: Low. (6-42 inches.)
Jump from Box: Medium
Depth Jump: High. Step from box, land, and jump high and vertically.
Upper body
Chest Pass : Low. But you can increase weight of ball.
Depth Push-up: Medium. Begin with arms extended on ball in a push-up position. Remove hands from ball, drop down, immediately push up to full extension. Quickly place palms on ball and begin again.
45 degree sit-up. Medium.
Drills with butt-kicker and stationary arm swing.
Periodization
Macrocycle�training season�could be nine months or four years in Olympics
Mesocycle: Several weeks to a few months
Microcycle: One week to four weeks with daily and weekly variations
Five kinds of mesocycles:
Hypertrophy: Muscular and metabolic base, high volume, low intensity, 2-4 weeks, 3-5 sets, 8-12 reps about 75% of 1RM with a one to two-minute rest
Strength: Sport-specific exercises of moderate volume and intensity, 2-4 weeks, 3-5 sets about 85% 1RM, 5-6 reps, 3-5 minutes rest
Strength/power: Integration of resistance and sport-specific power/explosive of low volume and high intensity, 2-4 weeks, 3-4 reps, 3-5 sets, 90%-93%1RM, longer rest, explosive exercises
Competition or Peaking phase: 1-3 weeks, Very high intensity, low volume, 1-2 reps around 95%, 3-5 sets, 3-5 minute rest.
Active rest: Rest a week then cross training, light work, and return to hypertrophy
Linear (from high volume, low intensity to low volume, high intensity or undulating on a weekly basis) and
Non-linear models�within the week microcycle vacillations�heavy, (85 to 95%) light,(65 to 75%) power, (30-95% explosive to core) moderate (75-80%)
A sample four day program could be heavy, light, off, power, moderate, mon-fri.
3 adverse outcomes for pregnant women:
1) insufficient oxygen or energy substrates to the fetus
2) hyperthermia-induced fetal distress or birth abnormalities
3) increased uterine contractions
Benefits:
• Improved cardiovascular and muscular fitness
• Facilitated recovery from labor
• Reduced postpartum belly
• Reduced back pain during pregnancy
• More energy reserve
• Fewer obstetric interventions
• Shorter active phase of labor and perhaps less pain
• Less weight gain
• Enhanced maternal well-being
• Increased likelihood of adopting permanent healthy lifestyle habits
• Perhaps avoid gestational diabetes
However, these benefits are all for the mother. There is also a lower birth rate, 10-12 ounces or 300 to 350 grams, and a 5 to 15 beat per minute increase in fetal heart rate with vigorous exercise. So perhaps moderate exercise would be better.
RPE: 12-16
No supine exercises after first trimester to avoid supine hypotensive syndrome.
Pregnant women may increase their minute ventilation by almost 50%, resulting in 10% to 20% more oxygen utilization at rest. Fetus can press on diaphragm as well. Avoid impact sports, downhill skiing, horseback riding. They need an extra 300kilocal a day to meet homeostasis. Hydration. Avoid heat.
CONTRAINDICATIONS
• Pregnancy-induced hypertension (preeclampsia)
• Ruptured membranes
• Premature labor during current pregnancy
• Persistent bleeding after 12 weeks
• Incompetent cervix dilating ahead of schedule
• Significant heart or restrictive lung disease
• Multiple-birth pregnancy that creates a risk of premature labor
• A placenta that blocks the cervix after 26 weeks
• Poorly controlled type I diabetes, seizures, hypertension, or hyperthyroidism
• Extreme obesity
• Extremely low body weight less than 12
• History of a very sedentary lifestyle
• Unevaluated maternal cardiac arrhythmia
• Severe anemia
• Heavy smoking
• Chronic bronchitis
• Orthopedic limitations
• Bloody discharge from the vagina
• Gush of fluid from the vagina
• Sudden swelling of the ankles, hands, or face
• Persistent, severe headaches, visual disturbances, fainting, dizziness
• Elevation of pulse or blood pressure that persists after exercise
• Persistent contractions (6-8 per hour) that may suggest premature labor
• Unexplained abdominal pain
• Insufficient weight gain�less than 2 pounds per month during the last two trimesters
Guidelines
• Perform 30 minutes or more of moderate exercise on most days of the week. ACSM
• Avoid exercise in supine after first trimester.
• Exercise should never continue past fatigue.
• Cycling and swimming are preferred to weight bearing or high risk activities.
• Cool environment, lots of fluid, loose, light clothing.
• Resume exercise gradually after birth.
Older Adults
Over 50, perhaps with cardiovascular disease, cancer, diabetes, osteoporosis, low back pain, arthritis, depression, obesity, and frailty. Resistance training decreases resting blood pressure 3 % or 4% and improves blood lipid levels, and can even be used postcoronary only with aerobic training. Exercise increases transit speed, which may reduce risk of colon cancer. Resistance training enhances glucose utilization, improves insulin response, and glycemic control, as well as preserving lean body mass offsetting muscle myopathy. Bone loss can be changed to bone gain through regular resistance training, mitigating the effects of osteoporosis and osteopenia. Strengthening lumbar extensors may alleviate back pain. Stronger muscles improve joint function and reduce debilitating pain. Strength training can alleviate depression and improve body image. Adults lose about one-half pound of muscle per year during their 30s and 40s and 1 pound after fifty, but the average aging American adds 4.5 kilos or 10 pounds of body weight which is 5-10 pounds less muscle and 15-20 pounds more fat, with a 2%-5% reduction in resting metabolic rate per decade.
Guidelines (These seem like suggestions for people over 70 or else medically compromised; otherwise human potential is diminished.)
• Resistance train 2-3 times per week on nonconsecutive days at 4-6 seconds per rep.
• Demonstrate first. Give verbal and kinesthetic cues, assistance, positive reinforcement.
• Aerobic training 2-5 days a week from 20 to 60 minutes, at 60% to 90% but 75% is best, unless on medication or compromised. Some may only do 5-10 minutes at 40%. They could have 30 beats above or below formulas even with a healthy heart, so perceived exertion may be better. 12-14
• Begin with aerobic activity, cool-down, stretching, then resistance, then stretching.
• Avoid lunges or step-ups.
Children as young as 6 can lift weights, and boys and girls have the same potential for strength because the testosterone blast has not yet begun; hence they have neural adaptations such as excitation-contraction coupling, myofibrillar packing density, and muscle fiber composition, motor neuron recruitment, rather than hypertrophy. Preadolescent youth can weight train but be careful of loading them during growth spurts. Their natural rhythm is sporadic bursts of moderate-to-high intensity followed by low intensity or rest. Use C-LPAM or the Children's Lifetime Physical Activity Model. Children optimally expend 6-8 kcal per kilogram per day. So a girl who weighs 88 pounds should expend at least 120 kilocal per day (3-4 minimum) and optimally 280 in physical activity. They can get increased bone mineral density, improved body composition, enhanced cardiorespiratory fitness, better speed and skill, and lower elevated blood lipids.
To avoid 50% of injuries youth should engage in more primary fitness activities pre-season.
Adults should supervise. One to three sets of 6 to 15 reps on single and multijoint exercises with 5% to 10% progression on two to three non-consecutive days.
To calculate BMI using non-metric units, Weight divided by heigh squared times 703 For example a person who weights 164 pounds and is 68 inches tall has a BMI of 25.
To calculate BMI using metric units, weight divided by height squared.
Weight: 78.93 kilo, and is 1.77meters tall =25.
78.93 divided by 1.77squared =25.
Underweight is less than 18.5, normal 18.5 -24.9, overweight 25.0-29.9, obese over 30, extreme obese over 40.
Gynoid obesity is pear-shaped in hip and thigh. Android apple is fat in trunk and abs, leading perhaps to Type II diabetes, hypertension, and CVD. Use waist circumference and BMI rather than calipers with obese.
A reduction in calories of 500 to 1000 a day will achieve a weight loss of 1 to 2 pounds a week. Total fat should not be more than 30%, protein 15% (lean meats and plants), carbs 55% or more, cholesterol less than 300 mg. 10% reduction of weight in 6 months.
1200 kcal, 800kcal�only with doctor's prescription.
Don't eat sweets, drink alcohol or soda, or processed foods.
Guidelines for Obese
Low impact aerobics �progress to five times 40-60 minutes, can begin with 2 daily sessions 20-30 min each or intervals. Get wide seats on bikes and ergometers. 40-70% VO2max. Weight train 2-3 times a week, 1-3 sets, 10-15 reps. Hold static stretches 10-30 s.
Disordered eating, anorexia nervosa, bulimia
Female Athlete Triad: Disordered eating, amenorrhea, (at least 3 consecutive cycles) osteoporosis
Signs for Bulimia
Vomiting at least 2 times a week for at least 3 months
Laxatives, enemas
Excessive exercise
Overconcern of body shape
Weight fluctuations of more than 10 pounds
Odor of vomit on breath
Scabs or scars on knuckles
Swollen puffy cheeks
Sore throat and dental problems
Abdominal symptoms
Erratic performance at work, school
Irregular or absent menses
Lacerations of oral cavity
Diarrhea
Constipation
Fatigue
Electrolyte disturbances
Heart irregularities
Ruptures in stomach
Signs for Anorexia
15% or more below expected weight range
Denial
Avoidance of social situations with food
Obsession with exercise
Sensitivity to cold
Layers of baggy clothing
Fatigue
Decline
Lanugo or baby hair over face and body
Yellow tint to skin
Loss of muscle mass and tone
Amenorrhea
Slow pulse�light headed on standing
Constipation
Encourage client to consume 200 to 400 kcal of complex carbs during first 30-90 minutes after exercise
Encourage a healthy diet
DO NOT EXERCISE EVERY DAY
Be careful of impact�stress fractures
See immediate medical attention for cardio-pulmonary irregularities
Hyperlipidemia
TLC diet. Less than 7% of saturated fats and less than 200 mg of cholesterol a day with lots of fiber and exercise.
<100LDL 130-159 Borderline high
Over 60 HDL is good.
Triglycerides <150 normal. 150-199 Borderline high
Metabolic syndrome is a cluster of major cardiac risk factors and abdominal obesity, also called syndrome X, dyslipidemic hypertension, and insulin resistance syndrome.
Waist cir: 40 inches in men, 35 in women
Triglycerides: >150
Less than 40 HDL in men and 50 in women
>130/86mmHg
Elevated fasting glucose .110mg/dL
22% of population has metabolic syndrome�heart disease and strokes.
DIABETES
Increased thirst, urination, appetite, and general weakness
Two fasting glucose levels of 126 mg/dL or higher, or two 2-hour postprandial plasma glucose measurements of 200mg/dL or higher after a glucose load of 75 grams.
Type I: Insulin-dependent diabetes mellitus
Pancreatic beta cell destruction by an auto-immune process, usually leading to absolute insulin deficiency. Approximately 10% of patients with diabetes have Type I. Must take exogenous insulin and are prone to ketoacidosis, which could lead to coma.
Type II: Insulin resistance in peripheral tissues and an insulin secretory deficit of the pancreatic beta cells, associated with family history of diabetes, old age, obesity, and lack of exercise. They can produce their own insulin however.
Gestational diabetes can occur during pregnancy. (2%-5% of pregnant women)
Exercise can increase insulin sensitivity and glucose utilization, lowering blood glucose levels. A complication could be hypoglycemia, lower than 65mg/dL, but be careful as soon as it approaches 70.
Stress cardiac testing by a medical pro must be performed for clients who are older than 35, or those who have had Type II for more than 10 years, Type I more than 15 years, or with evidence of microvascular disease like retinopathy or nephropathy. Other contraindications are glucose over 240 in Type 1, 300 in Type II, loss of sensation in feet (may be able to swim or bike), and acute illness, infection, or fever.
The biggest deleterious side effect of exercise could be hypoglycemia from increased intensity, longer time, inadequate fuel beforehand, insulin injection into the exercising muscle, or severe cold. Hypoglycemia �loss of concentration, shaking, shivering, sweating, tachycardia, loss of consciousness. So have juice, bananas, oranges on hand.
Glucose levels should be monitored before and after exercise, as well as every 30 minutes. Snacks are okay if levels are low, but wait a few hours after a meal.
PROGRAM: 4-6 days a week, for 20-60 minutes at 40% to 70% of VO2 max (aerobic)
Resistance train 1 set, 8-12 reps, two to three times a week
5-10 minute warm-up and cool-down, hold static stretches 10-30 seconds
Over 50 million Americans age 6 and over have hypertension�over 140-90, 90% are idiopathic, only 10 curable if caused by hyperthyroidism, pheochromocytoma, hypercortisolism, hyperaldosteronism, and renal artery stenosis. They must have medical evaluations for target organ damage or cardiovascular disease. You don't feel it till it is too late�chest pain, visual blurring, neurologic deficits, i.e. strokes or heart attacks.
High Normal 130-139/85-89: Lifestyle modification for Groups A and B, drug therapy for those with heart failure, renal insufficiency, or diabetes, and lifestyle modification
Stage I 140-159/90-99: Lifestyle modification up to 12 months for Group A, 6 months for Group B, and drug therapy for Group C and lifestyle modification
Stages 2 and 3 160/100: Lifestyle modification, drug therapy
Goals are to bring it to as low as 125/75 for people with renal failure with proteinuria
Blood pressure has decreased 4/5/3.8mmHg with long term-resistance training, and 4.7/3.1 with aerobic training.
Program: Sleep, limit salt and alcohol, get enough potassium, aerobic 30-45 minutes four or more days of the week, stop smoking, and reduce dietary fat and cholesterol
Drugs include beta-blockers, alpha-blockers, and calcium-channel blockers, possibly diuretics. The blockers can cause blood pooling so there should be a longer cooldown. Must use RPE as heart rates are not reliable.
PROGRAM: Low-intensity exercise at 40%-50% of maximal oxygen uptake is efficient for reducing stress. RPE of 8-10 on the 6-20 scale with a goal range of 11-13, between 15-30 minutes then going to 30-60 minutes, 3-7 days a week, weekly caloric expenditure of 700-2000 kilocal in 4-6 months. Resistance should begin at 16-20 per set, 50% to 60% of 1RM, with a 2-3 minute rest between sets. Can do 1-3 sets. Over time you can move to 6-12 reps. Two to three times a week, between 30-60 minutes. Goals are to increase VO2max and ventilatory threshold, maximal work and endurance, caloric expenditure, blood pressure, and muscular endurance.
If a client suddenly comes to class with a Stage I pressure, you must cancel the session and have him see the doctor. Don't treat post MI clients with CAD and no angina because they may die on you all of a sudden.
Be careful of comorbid conditions such as musculoskeletal, neurologic, and vascular.
PROGRAM FOR MI:Begin at 40% of VO2max or RPE of 9-11, 15-40 minutes 3-4 times a week. Additional time for warm-up and cooldown. Resistance begins at 20 reps, 1-3 sets, 2-3 days a week. Treadmill is okay.
PROGRAM FOR POST CVA: Consult CVA medical team. Ergometers may be more important than treadmills because balance is usually off. Can begin as low as 30% VO2max�they can be so deconditioned, you have to measure peak VO2. Eventually they may do 40%-70%. Session can be 5-60 minutes, 3 times a week. Resistance training is crucial to develop new pathways, and perhaps have a crossover effect on the compromised limb. Eventually do 3 sets of 8-12 reps two to three days a week. Daily ROM needed (even 5 minutes) to avoid contractures. Do balance and coordination exercises.
PROGRAM FOR PVD: They can't walk for more than 2-5 minutes because of the searing pain in their calves. They may take nitroglycerin for chest pain with a bitter taste and soon-to-follow headache. If client has pain, ache, dyspnea, sit him down, take nitro, and call EMS . Claudication is the rate-limiting factor. So walk till it hurts, stop, rest, do it again, and try to proceed to 10-30 minutes. Low-intensity exercise at 40%-50% of maximal oxygen uptake is efficient for reducing stress. RPE of 8-10 on the 6-20 scale with a goal range of 11-13, between 15-30 minutes then going to 30-60 minutes, 3-7 days a week, weekly caloric expenditure of 700-2000 kilocal in 4-6 months. Resistance should begin at 16-20 per set, 50% to 60% of 1RM, with a 2-3 minute rest between sets. Can do 1-3 sets. Over time you can move to 6-12 reps. Two to three times a week, between 30-60 minutes. Goals are to increase VO2max and ventilatory threshold, maximal work and endurance, caloric expenditure, blood pressure, and muscular endurance
Clients with severe angina and COPD must exercise in a medical setting.
Asthma: is reversible airway disease with associated hyperreactivity, characterized by the ease of developing bronchospasm, constriction, or both. Some severe forms require stronger meds (inhaled and oral steroids usually for late stage airway edema) than the inhaled bronchodilators for early stage bronchoconstriction. Status asmaticus is an acute mucus plugging of the airways.
EIA: Self-limited, can begin 5-20 minutes into a session, and has associated coughing, wheezing, or both.
PROGRAM: RPR and sense of shortness of breath. Those taking steroids may have muscular disease of the respiratory muscles. Better with mid to late morning exercise because of the natural daytime release of cortisol from the adrenal glands. Avoid temperature extremes. May not achieve THR but some physiological improvements will occur. RPE 11-13, 1-2 times daily, 3-7 days of the week, 30 minutes, but can begin 5-10 minutes. Resistance training can be 16 reps, 2-3 days a week. Flexibility, core strengthening and stretching etc.
Injuries can involve macrotrauma or sudden onset, or microtrauma or insidious onset, which can relate to poor program design, suboptimal training surfaces, faulty technique, insufficient motor control, decreased flexibility, or skeletal malalignment.
Go from a acontusion, to a first, second, (partial), and third degree muscle strain (complete tear), tendonitis, tendinopathy, joint sprain (first, second, and third degree tear of ligaments), bone fracture, (avoid stress fractures through excessive training on hard surfaces), subluxation, or dislocation (partial or complete displacement of joint surfaces).
Inflammation: Histamine and bradykinin increase blood flow and capillary permeability causing edema which inhibits function. Two to three days after an injury, but much longer after surgery or severe structural damage. RICE
Repair:3-5 days after injury up to two months. Damaged tissue regenerated as scar tissue. New capillaries, connective tissue, collagen fibers parallel and longitudinal to the line of stress. If fibers are laid down incorrectly, transverse friction is good. Prevent muscle atrophy and joint degeneration, promote collagen synthesis, avoid disruption of newly formed collagen fibers. Low-load stresses. Avoid resistive exercises of damaged tissue, except submaximal, pain-free, isometric exercise.
Remodeling:Increased loading allows collagen fibers to hypertrophy and align themselves along lines of stress. Can last 2-4 or more months after surgery. Add more advanced, activity-specific exercises that allow progressive stresses to be applied to the injured tissue.
Organize a program with indications and contraindications, such as avoiding the last 30 degrees of extension after an ACL graft, or a precaution, which requires supervision.
Disc injury: Part of nucleus pulposus burst through annulus fibrosis, resulting in inflammation and nerve damage if it damages the spinal canal. Client may feel pain or weakness into the buttocks (sciatic notch), down the legs or even have a foot drop in severe cases. Excessive flexion is contraindicated, because it may push disc contents further towards spinal canal. Avoid full sit-ups, full or loaded squats, (although plies are okay), rowing movements, and the deadlift. Watch excessive flexion on the bike, the rowing ergometer, or aerobic dance, toe touches. Do gluteal, hip adductor, and upper back stretches under supervision�precaution. Avoid knee to chest, spinal twist stretches, extreme flexion/rotation, especially passive assisted or resisted. (Psoas and piriformis stretches are okay if isolated).
PROGRAM: passive lumbar extension, isometric abdominal and extensor strengthening progressing to lumbar stabilization
Muscle Strain: Traumatic tears require three-stage tissue healing, avoiding elliptical, rows, power etc during early stages) while insidious tears postural retraining. Avoid exercise during inflammatory period, progress to gentle flexion stretching, followed by extension strengthening.
Spondylolysis (a defect or fracture of the pars interarticularis region of a lumbar vertebra) and spondylolisthesis (its progression into a forward slippage of one vertebral body on another) often occurring in lumbar extension injuries such as football, accidents, diving etc.: Avoid hyperextension, extend only till neutral, avoid squat, shoulder press, and push press with heavy weights, although these movements can be done with nothing, provided posture is good. Do ab crunches and knee to chest. Avoid hyperextension with spinal stenosis, and try to decompress with water activities in a good posture.
Shoulder: Impingement syndrome: Pinching of the supraspinatus, the long head of the biceps, or subacromial bursa under the acromial arch. Strengthen rotators, stabilize scapula, correct posture, fix glenohumeral rhythm, may begin with decline bench press, do lateral raises in external, not internal rotation, avoid upright row, Versaclimber, and be careful with ball sports
Anterior instability: The humeral head moves too far forward, resulting in possible injury or dislocation. Following a dislocation of the shoulder, redislocation can occur in as many as 90% of young, active people while only 30% to 50% of middle-aged. Surgical management can include arthroscopy, or high tech instruments that shrink the joint capsule (thermal capsulorraphy) to assist in stabilizing the head. Movements that involve greater than 90 degrees of elevation, placing the hands and arms behind the plane of the shoulder may lead to redislocation. The safe zone is below 90 degrees of elevation anterior to the frontal plane of the body. These modifications must be permanent, including avoidance of the freestyle, backstroke, and butterfly, and some racket sports, hands behind back stretch and behind neck stretch.
Rotator Cuff debridement and subacromial decompression: Debridgement means to scrape away at the edge of a tear until a clean, bleeding surface of tendon is achieved. SAD involves scraping or shaving away the bone on the anterior and inferior surfaces of the acromion to decrease the stress or impingement of the rotator cuff tendons between the acromion and head of the humerus. The shaved bone often takes 12 weeks or more to heal, creating significant amounts of pain. ROM and gentle PT begin immediately. 4-6 weeks after surgery clients can perfom rotator cuff exercises, and by 6-8 weeks PT is over. They should continue rotator cuff and scapular strengthening. Contraindications include high-resistance, low-rep upper extremity strength training, and exercises outside the safe zone, and full ROM shoulder press, bench press, pec dec, and behind the neck pulldown. Avoid throwing, swimming, and racket sports.
Rotator Cuff repair: Surgical repair after a tear that is full thickness, particularly supraspinatus�could involve open incision as well as arthroscopy. Greater periods of immobilization in a sling (2 days to 6 weeks, depending on age, tissue quality, and presence of additional injuries. Follow shoulder protocol, but immobilization requires ROM in rotation and abducition.
Strengthen rotators side-lying, then prone shoulder extension, prone horizontal abduction (rear delt flys), prone 90/90 rotation and then standing rotation (light weights, high reps�15-20)
Stabilize scapula�upper and lower traps, serratus anterior, and levator scapula
Knee: Chondromalacia, iliotibial band friction syndrome, irritated plica, patella tendonitis caused by overuse, including surfaces and gear, biomechanical faults, (patellofemoral malalignment, improper patellar positioning, tightness of lateral retinaculum or ITB, or excessive pronation or supination) and muscular imbalance (relationship between VMO and vastus lateralis). Quads help clients walk up and downstairs and decelerate on level surfaces. However, deep squats or knee flexion beyond 90 degrees increase compression between patella and femur and should be avoided so high impact, step are contraindicated in favor of cycling and water exercise to reduce inflammation in anterior knee pain.
ACL: Limits anterior tibial translation and rotation relative to the femur. ACL reconstruction has improved. Two different kinds of grafts�the semitendinosus/gracilis grafts preclude immediate postoperative active or resistive knee flexion exercise until 4-6 weeks following surgery. At discharge�4-6 months from PT clients should have good strength and ROM. Translation of the tibia relative to the femur is minimized because of the weight bearing and muscular co-contraction during closed kinetic chain exercises which allow multiple joints to be exercisesd. While both open and closed chain should be performed, the greatest amount of anterior tibial translation occur in the final 30 degrees of leg extension in an open kinetic chain. Safe zone is 90 to 45 degrees of extension for six months to one year after ACL. Use of unilateral stance, single-leg squats, and step-ups insures that clients will not favor injured leg. Shallow steps, biking, and swimming are preferred for aerobics.
TOTAL KNEE ARTHROPLASTY: Re: Degeneration and degradation of joint surfaces of distal femur and proximal tibia, excessive valgus or varus, fractures, meniscal pathology, instability. Following discharge, patients have 100 to 120 degrees of flexion and nearly complete extension. Cycling, swimming, endurance with reduced impact, leg press, multidirectional hip strengthening, calf raises, flexion and extension low resistance high reps are recommended. Avoid kneeling or lunges performed too deeply. Focus on ROM.
TOTAL HIP ARTHROPLASTY: To relieve osteoarthritis, cemented (immediate post-operative weight-bearing) and uncemented, (weight-bearing restrictions 6-12 weeks) lasting at least 15 years with techniques posterior, (risk of dislocation) anterolateral, and transtrochanteric. No hip flexion greater than 90 degrees, no hip adduction past neutral, no hip adduction machine, no hip internal rotation, high impact, resisted hip flexion, full sit-up. Do ½ squats, elliptical, and improve gait.
ARTHRITIS: OA�mechanical stresses leading to microfractures, deterioration of weight-bearing cartilage, proliferation of new bone at margins of joints like spurs or osteophytes, and sclerotic changes in subchondral bone. In majority of people age 55 and older. Chondroitin sulfate and glucosamine. Biking, elliptical, swimming, weight management. Open chain upper body, no push-ups, and lower body except full ROM with patellofemoral syndrome. Light weight closed kinetic chain for lower body.
RA- inflammatory, autoimmune, proliferation of joint's synovial lining, pannus, edema, inhibition. Exacerbation, remission, then progression. Unstable joints. Disuse atrophy. Can include osteoporosis, periarticularnodules, deformity, ankylosis. Neck, shoulders, wrists, and hands. Don't do high impact, neck exercises (particularly resisted) or movements outside the safe zone, upper trap stretch, behind the neck shoulder press. (Could rupture ligaments of neck, rotator cuff tears in 30% to 40% of RA, loss of grip strength.) Exercise at 60%-80% on bike, (vigorous non-impact aerobics may reduce inflammation), elliptical, stepper, ROM but don't overstretch, isometrics, stationary bike, water aerobics. May have to build up dumbbell's diameter to facilitate grip. During acute flare-ups, rest.
Spinal Cord Injury: Between T-1 and C-1�quadriplegia or tetraplegia, complete paralysis. T-2-T-12�paraplegia of trunk, legs and or pelvic organs. Thromboembolic events and dysrhythmias, reduced vascular tone, and unbalanced hyperactivity of the vagal system. High lesions are prone to bradycardia, primary cardiac arrest, and cardiac conduction disturbances. Chronic CVA could has atherosclerosis, angina, heart failure and other serious cardiovascular manifestations, particularly AD or autonomic dysreflexia, which is a disruption in normal neural regulation of arterial blood pressure, esp above T6 where there is hypertension (20-40mmHg or boosting) due to distended bladder, menses, sores, sex, scrotal compression, restricted clothing, infections�can die. Look out for pounding headache, sweating, goose bumps, blurred vision with spots, congestion, anxiety and dysrhythmias. Track wheelchair and swimming athletes with SCI sometimes strive for AD to boost their circulation and get this reflex response. Overuse injuries are at shoulders, wrists, and elbows�57% of NWAA. So stretch anterior and strengthen posterior compartment. Higher HR and lower BP compared to others. Above T-6 clients cannot regulate through sweating or shivering. Compensate or work only in temp controlled environments. Risk of dehydration and poor venous return as well. Train in supine position, be alert to fainting. Also at risk for CVD, diabetes, dyslipidemia etc. They may not know they are having a heart attack. Limited by extensive paralysis and or sympathetic autonomic nervous impairment.
Multiple Sclerosis: Autoimmune disorder, related to Epstein-Barr virus, sensory disturbances, fatigue, weakness, ipsilateral optical neuritis, gait ataxia, neurogenic bowel and bladder, trunk and limb parestheisa. 80% have relapsing/remitting and 20% have progressive MS. Benign (10-15%) Minimal or no disability, Classical relapsing-remitting (25-30%) , Chronic relapsing-remitting (25-30%), often permanent motor and sensory deficits, chronic progressive (15-20%) insidious onset, gradual but steady worsening of symptoms, quadriparesis, cognitive decline, visual loss, loss of bowel, bladder, and sexual function. Manage dystonic spasms, spasticity, ataxia, incordination, depression, dysfunction, pain etc. Could have foot drop, memory problems. Meds manage inflammation and try to modify disease process. Although sedentary, aerobic exercise could increase fitness 30%. 40-70% of VO2max or HRR, progressing over 3-6 months to 50-70% as tolerated. Yoga, tai chi, resistance with modifications. Prone to heat intolerance, but could do aquatics if it isn't too hot. 8-12 exercises, 40-60% of 1RM load , 1-3 sets or 8-12 reps. Progression at 50% of normal rate.
Epilepsy: Two or more unprovoked, recurring seizures�involuntary alteration in movement, sensation, perception, cognitive behavior, and or loss of consciousness. Status epilepticus is a seizure lasting more than 30 minutes or so frequently that consciousness is not restored. Recognize precipitants�exercise could do it in 10% of the cases, emotional stress, hyperventilation, menses, sleep deprivation, fever, lights/TV, alcohol, then modify intensity or avoid exercise. Partial seizures can be: Simple with no LOC, Complex (35-40%) partial or complete LOC, often preceded by aura, evolving to generalized (40-45%) including both hemispheres, complete LOC. Generalized seizures can be petit mal (staring or eye flickering), no convulsions, myoclonic, clonic, tonic, tonic-clonic (or grand mal, which is rigidity followed by flexion with labored breathing, tongue biting, cyanosis, incontinence, post-ictal confusion, fatigue, stupor) or atonic, loss of postural tone. A weight loss of ten pounds can increase the bioavailablity of antiseizure medication, and risk of side effects. First aid: Keep client prone. Remove glasses, loosen clothing, do not restrain, keep objects out of path, do not place anything in mouth, after seizure, turn client into CPR recovery position, observe until awake, alert doctor and family.
Cerebral Palsy: Impaired body movement and coordination (apraxia, ataxia from cerebellum, athetosis from midbrain, chorea, dyskinesis from basal ganglia, dystonia, myoclonus, spasticity from motor cortex of cerebrum) with possible difficulty swallowing, speaking, or seizures (60%) etc due to brain damage at birthing or infancy, but it isn't progressive. CP1-8 from severe spastic tetraplegia to minimally affected diplegia. Excellent responses to exercise. After medical clearance, can do arm and/or leg ergometer, rarely treadmill can be used if they have balance. Wear gloves or strap feet to pedals. 6-12 minute walk or wheelchair push. Skinfold measurements can be taken at uninvolved sites. 50-85% VO2 or HRR, 30 minutes, 4 or more days of the week. Begin with 5-10 minutes twice a day. May not be able to use free weights�just machines. Warm-up, cooldown, and stretching. Cognitive, visual, hearing, and speech difficulties. Supervise on machines like treadmill, ski, elliptical.
Facility organization can be by body part, or by equipment type.
• Equipment that requires spotters should be located away from windows, mirrors, and doors.
• Tallest machines or power racks should be placed along walls, and may need to be bolted. Dumbell racks also on walls and shorter, smaller pieces in the middle.
• Resistance training machines are placed in an order so that large muscles are trained first, smaller ones last.
• Stretching is a separate area, with a minimum of a five foot user length and width for a home gym.
• Aerobic machines that require clients to be upright (treadmills, elliptical) should be placed behind the rowing machines and bikes so that the taller machines are close to the wall.
• All equipment should be placed at least 6 inches (15 centimeters) from mirrors, which should be 20 inches above the floor.
• Separate room for group exercise.
• Bench press, lying triceps extension: 156 square feet
Standing exercises like biceps curl and upright row: 100 square feet
Back squat and shoulder press: 100 square feet
Olympic lifting platform with 4-foot safety space cushion and lunge and step-ups: 256 square feet, 36 inches between the ends of the Olympic bars
Stretching and warm-up: 49 square feet, larger if PNF is needed
Treadmill: 117 square feet
Machine seated chest press: 110 square feet
Aerobic dance videotape: 36 square feet
Traffic flow should be around perimeter of machines. There should be at least one walkway that bisects the room, three feet wide maintained clear at all times. Ceiling should be free of low-hanging apparatus and high enough for jumping�minimum of 12 feet. All resistance training machines should be placed at least two feet, preferably three feet apart. If a free weight exercise is performed, a three-foot safety space cushion is needed between the ends of the barbell and adjacent stations, as well as between multi- and single stations. The ends of all Olympic bars should be spaced three feet apart. A free weight station should be able to accommodate three to four people. Racks holding the fixed-weight barbells should have a minimum of three feet between the ends of the bars. Weight trees should be placed close to plate-loaded equipment, but not closer than three feet. The walkway around Olympic platform should be three to four feet wide. Three feet is a good cushion around everything although a small home gym may only have 18 inches, with 25-49 square feet for aerobics.
Ground electrical equipment and outlets, keep facility free of children and pets, machines should not exceed home circuitry. Lighting, circulation, flooring, (rubberized, wood, tile, padded, short-pile, or aerobic platforms) mirrors 20 inches off the floor. Plyometric boxes and jumping equipment must have padded flooring, nonslip surfaces.
PTs must inspect, clean, and maintain equipment. Guide rods on selectorized machines should be cleaned and lubricated twice a week.
Be able to calculate the total needed area in square feet if client is performing seated shoulder press, upright row with a 5-foot long bar, a 5-foot long weight bend for the lying triceps extension with a 4-foot EZ-curl bar, a step-up on an 8-foot Olympic platform with a 3-foot safety space chsion, a front squat in a41/2 square power rack using an Olympic bar, a stair machine, and a seated toe touch.
LAW
Understand contracts and torts resulting from negligence�a failure to act, or substandard care. Many PTs do not have appropriate education, training, and certifications, and there is no licensure as there is for massage and physical therapy. It is crucial to keep records of comprehensive assessments, appropriate fitness tests, thorough evaluations, suitable program design, attentive supervision, emergency prep. Only NSCA and ACSM have credible certifications for personal training and formal education in the exercise sciences is crucial. Know the difference between common or case law based on past cases, and statutory law, enacted and authorized by statutes, ordinances, and codes. Usually PTs are sued in a civil suit, but criminal action could occur with the unauthorized practice of an allied health profession, even with the attempt to prescribe rehab or dietary recommendations. Contractual requirements are established when it is documented that a written agreement existed, consensual words were articulated, or that implied conduct was expressed, as well as releases, waivers, assumptions of risk, informed consents, or any exculpatory agreement. Contracts are also between business partners�any fiduciary relationship. A tort necessitates the establishment of a legal duty coupled with the fact that breach of that duty resulted in proximate cause of a verified insult, injury, or death to which compensation can be awarded, which can be intentional or negligent or strict liability regardless of fault such as defective equipment produced by the manufacturer. If a primary settlement cannot be achieved, then the plaintiff and defendant go through the discovery process where all paperwork is inspected and analyzed such as contract, medical history, lifestyle questionnaire, physical exam reports, physician clearance forms, informed consents, waivers, releases, assumption of risk forms, fitness profiles, program design, workout logs, personal notes, as interrogatories and depositions are taken of all involved, especially PT's education and credentials. An incident report must be filed immediately, especially if it happens at home. Someone other than trainer should have witnessed client's signature, and all forms must be updated every year, and stored for at least four years.
First a summary judgment is sought to dismiss the case. An arbitration hearing is held in hopes of again settling out of court; if it doesn't work, a jury trial begins for adjudication. Employers can be found vicariously liable for negligent acts of PTs (even as independent contractors) in respondeat superior. You can be sued for negligence, (protect with a waiver�exculpatory clause) inherent injuries (no one's fault so protect with an informed consent or agreement to participate), and extreme forms of negligence. If an exculpatory clause is added to an agreement to participate for adults then it becomes a waiver. Negligence can be as simple as not completely a PAR-Q form or perceived sexual harassment. But the plaintiff must prove duty (standard of care), subsequent breach of duty, causation, and damages, which can be compensatory (and comparative or contributory depending on whose fault it was) or punitive. Expert witnesses are usually other trainers or health professionals.
Memorize the following liability exposures:1)Preparticipation screening and clearance
2) Personnel qualifications
3)Program supervision and instruction
4)Facility and equipment setup, inspection, maintenance, repair, and signage
5)Emergency planning and response
6)Records and record keeping
7)Equal opportunity and access
8)Participation in strength and conditioning activities by children
9)Supplements, ergogenic aids, and drugs
Code of ethics cements the standard of care with confidentiality, respect, continuing education, a safe and effective environment, and reporting other people who violate this, avoiding words diagnose, or treat, in favor of assess, motivate, educate, train, and refer unless they have other licenses that permit this. Exercise program, not prescription. Must monitor signs and symptoms of overexertion, intensity levels, and proper form and execution of movement. Fitness owners are business invitees who must maintain safe premises. Clients injured on equipment can sue PT, manufacturer, facility or all three. Even at home, what is the emergency plan? Kits must be inspected once a month and rehearsals quarterly. Need AED as well�over 95% of CVA die without it, because once blood stops circulating, every minute without defibrillation decreases the chances of survival 10%.
With a mild to moderate MI, activate EMS , and administer emergency oxygen.
Arm stroke accounts for 80% of power in freestyle.
17% body fat is lean for a 46 year old male.
Don't grasp the patellar tendon insertion in a knee to chest stretch.
A common technique in back hyperextension on the stability ball is allowing the navel to move off of the ball.
Rowing machines is the cardio machine that works the most muscles.
On free weight bench press keep wrists rigid below elbows, and don't extend bar upward and slightly away from the face.
Depth jump is the highest intensity plyo.
Incorrect technique can help perform more repetitions more easily but hurt the body and not achieve results.