(Copyright 2005)<julia.keefer@nyu.edu> Dr. Keefer is a kinesiologist, massage therapist, fitness instructor, and creator of four trademarked classes.
PART TWO: Dr. Keefer's Corrective Clinic: Lower Body
Pre-hab and Rehab for Happy Hab!
This section is an introduction to basic body sculpting for Level I as well as a way for Levels II and III to make the transition from physical therapy to optimal functioning. It also gives you preventive exercises so you can avoid problems before they occur.
Why do people get injured?
Too much too fast
Not enough strength for the activity
Muscle imbalances
Obesity
Asthma or other cardio-respiratory problems
Excessive impact in sports
Arthritis or other pre-existing musculoskeletal conditions
Improper equipment
Now that something isn't working right, what can you do about it?
The body has to go through its natural cycle of inflammation, proliferation and remodeling in order to heal. Decreasing inflammation with ice and elevation is fine, but avoid any stress to the injured area until the inflammation is over. However too much swelling, pain and faulty gait and alignment may cause permanent damage.
If you have tendonitis, ice-and-stretch, rest, and slowly strengthen the belly of the muscle with isolated weight lifting.
Ligamentous and meniscus injuries are more problematic. While physicians have developed a number of twist and traction or compression tests like the Apley, the McMurray, the Anterior Drawer, it is usually best to just get an MRI and see what is going on.
Don’t diagnose yourself or get friends to diagnose you. After the diagnosis, pursue medical treatment and physical therapy, and then graduate into the Keefer clinic.
Physical therapy exercises can be done every two or three hours, or just once a day.
Each clinic chapter is divided into posture or alignment, pathologies and injuries, exercise, massge, ideokinesis, and aerobic activities. The goals of a complete rehab program are to regain strength, power, endurance, flexibility, balance, and heart and lung fitness. Not all exercises are appropriate for every injury, so make sure your doctor circles the ones you need. Stop any exercise that causes significant pain during or after exercise, another reason why you shouldn't take pain-killers before workouts, if you can help it.
Discuss frequency with your doctor as well. Postural re-training exercises for bad backs can be done in the morning and evening, quad setting for injured knees is sometimes done every few hours, but strength training with weights is only done every other day.
Don't follow templates blindly; remember that everything you depends on something else.
PRICE
Protect, Rest, Ice, Compression, Elevation
Isometrics
Stretch around it
Strengthen antagonists
Strengthen injured muscles
Full body no-impact aerobic activity
Balance muscles
Re-integrate injured area
Breathing
Exhaling on the exertion is the safest thing to do for the heart. Inhaling and then lifting a heavy weight raises the blood pressure. On the other hand, expanding the chest and holding a deep breath fills the lungs, which supports the rib cage and prevents the chest from collapsing forward. This, combined with simultaneous abdominal and back contraction, maintains the solid core to lift heavy weights. Imagine your chest like an accordion, opening and closing, as your belly and back expand and contract. Use all dimensions of the upper and lower torso to breathe, focusing first on diaphragmatic breathing.
Performance
While sports and dance require a wide dynamic range, use a slow, controlled effort in the clinic, varying the tempo to stress the positive or negative strokes of the motion.
Once you are healed completely, then you can graduate from the Clinic and do more athletic activities gradually increasing speed, size, complexity, and trajectory of motion.
Muscles and Movement
Here is a chart demonstrating the principal actions of flexion, extension, abduction, and adduction. 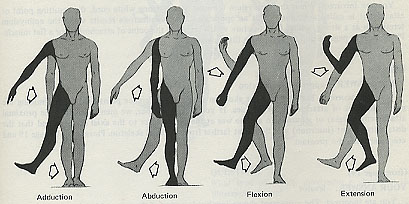 But Dr. Keefer's rehab secret is to work the small muscles and internal and external rotation, particularly of the hips and shoulders. Don't be superficial about your exercises. Get to the core, even if it is a chore. And the body moves in all kinds of mysterious, indirect ways, even if it happens when you are sleeping.
But Dr. Keefer's rehab secret is to work the small muscles and internal and external rotation, particularly of the hips and shoulders. Don't be superficial about your exercises. Get to the core, even if it is a chore. And the body moves in all kinds of mysterious, indirect ways, even if it happens when you are sleeping.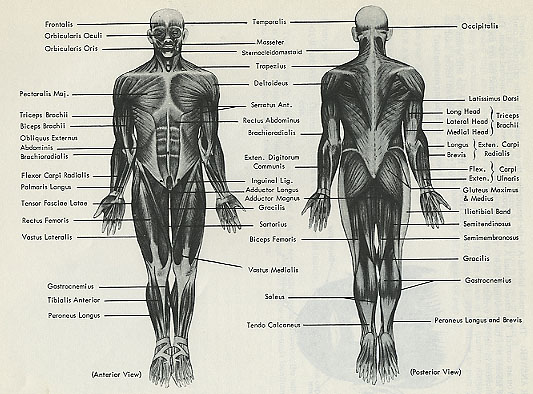 These are the superficial muscles, but are you working the deep ones?
These are the superficial muscles, but are you working the deep ones?
Ch07: My Feet Hurt!
Alignment
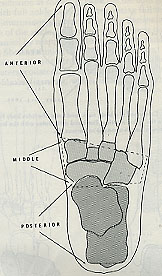
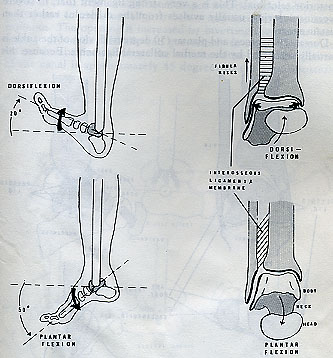
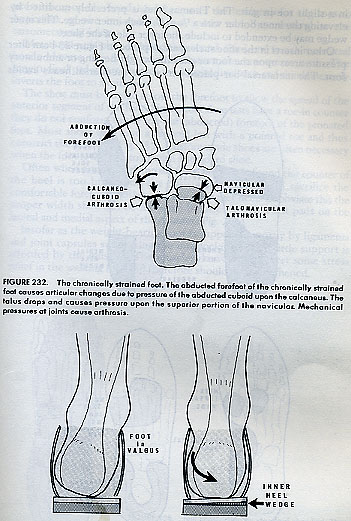
Pronation combines eversion, abduction, and dorsiflexion, while supination combines inversion, adduction, and plantar flexion.
The ankle can dorsi or plantar flex, evert or invert, but all the digits of the toes have their own articulation, just like the hands. If trained from birth, your feet could type at the computer.
Orthotics
A good podiatrist can help realign your foot with orthotics. But to avoid stiffness, take those shoes off every night and move your feet around, pick up pens, draw your name, stretch your calves, and flex your ankles.
Problems
The foot has 26 bones that can splinter, fracture, get deformed, or calcified. Therefore if you have pain, always get an MRI.
Although you may not know the medical names, you may have the following complaints:
Numbness, burning, infection, skin rash (local or radiating from above?)
Pain on the bottom of the heel when you step on it (plantar fasciitis?)
Painful cramp between third and fourth toes when wearing shoes (Morton’s neuroma?)
Thickened, streaked or discolored toenails
A large bump beside the big toe that is always red (bunion?)
Thick corns
Swollen ankles
Bunions
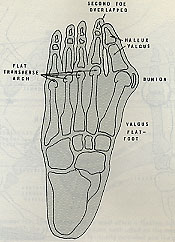
Hallux valgus is lateral deviation of the proximal phalanx upon the first metatarsal which can be accompanied by enlargment of the medial portion of the first metatarsal head, and inflammation of the bursa over the medial aspect of the metatarsophalangeal joint. Bunions are common but don't have to hurt if your feet are strong and flexible and you wear wide shoes that don't cramp your toes.
But hallux rigidus can be painful. Try to prehab this condition by keeping the feet flexible. In normal gait every step causes the big toe to hyperextend during the last phase of stance as the body moves ahead of the center of graity. Walking is impaired if the metatarsophalangeal joint is rigid. If they start to get stiff, move them while swimming in a pool or bathing in a warm tub.

Hammer Toes is a fixed flexion deformity of the interphalangeal joint with hyperextension of the metatarsophalangeal join. A painful callus can form. Church-and-steeple exercises can help prevent it unless it is congenital.
Morton’s Neuroma
A short first metatarsal bone causes excessive weight to be borne by the second metatarsal. Over time you may feel pain at the base of the first two metatarsals and at the head of the second. Eventually this can swell into a neuroma, a fusiform swelling of a digital nerve, between the second and third or third and fourth toes. Orthotics, digital separation, strengthening and mobility are preferable to last-resort surgery.
Plantar Fasciitis
Plantar fasciitis is inflammation of the fascia on the sole of the foot and can be the forerunner of a calcaneal spur. To prevent this, roll through, stretch, and strengthen the feet. But if it happens, then you may have to ice, rest, and tape it till it heals. With this condition, it generally hurts most in the morning when you first put weight on it. Therefore, if the condition continues, try a night splint to keep the ankle in dorsiflexion, and prevent the fascia from cramping up. Like a tennis elbow, it must be permanently corrected through a alignment, stretching, and strengthening and program so that your feet have the ability to withstand the stresses to which you subject them. I can usually relieve the pain with ultrasound, followed by deep tissue massage. If you are a runner, cross-train with biking and swimming until it clears. If you have been jumping, go back to a ballet barre and really strengthen your feet.
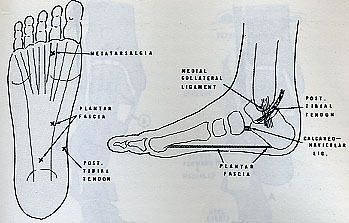
Metatarsalgia
Metatarsalgia is a condition where there is pain and tenderness of the plantar heads of the metatarsals, which often happens when the anterior transverse arch is depressed or if you have excessive weight on the heads. A pronated foot can have metatarsalgia.
Often people with the highest insteps get metatarsalgia because the arch gives out here allowing the toes to flap around like galoshes. Use a metatarsal arch support in your shoes and strengthen these muscles by dorsiflexing the ankle and picking up pencils or playing the church and steeple with your fingers and toes to avoid curling your toes.
Sprains and Strains
Spraining your ankle, an inversion sprain, can be fixed by PRICE for a week, with gradually mobilization and strengthening exercises. Don't forget to regain your balance with BAPS so it doesn't happen again. If you think you are about to sprain your ankle, quickly turn your toes to the sky to dorsiflex so that it doesn't invert.
The most dramatic is an Achilles tendon rupture which can come on suddenly in sports or insidiously in weakness and old age. Either way, it can put you out of commission for more than six months. Always stretch and strengthen the Achilles turned in and turned out, slowly and quickly. For sports strengthen your soleus and toe flexors and extensors to share the impact. When you start to get Achilles tendonitis, stop and recover--don't push it to its breaking point.
The feet are often your only direct contact with gravity and yet they are ignored in most exercise programs because people focus on the big muscles or the areas where fat accumulates. Feet can’t get fat and so far no one gets turned on by a bulging flexor digitorum longus. However, strong feet allow us to run, jump, turn, climb, and even walk into advanced years. When your feet hurt you can’t even go outside and have fun or stand up comfortably at a party.
Avoid heels and pointed toes as much as possible, except if you are sitting at a dinner party. Get athletic shoes that allow you to walk comfortably. There are motion control shoes to combat overpronation, when the arches turn inwards, neutral and then flexible shoes for supinators, people with high, rigid arches.
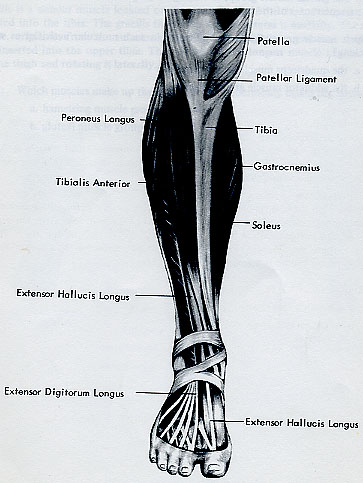
Muscles
The extrinsic muscles originate from the lower leg, the gastrocnemius soleus group to plantar flex the foot and invert the forefoot, the lateral or peroneal muscles to evert the foot, the medial or posterior tibila muscles to invert as well as plantar flex, and the anterior group or tibila muscles to dorsiflex and supinate the forefoot.
The intrinsic muscles stop and start in the feet themselves and include the short versions of some of the above muscles, and the muscles that puff up the arches from below, support them from above and move the toes around. I didn't realize how important the feet are until I started taking ballet class at 30 years of age. At first they hurt all the time but when I got stronger I excelled at every sport and now the feet are the first thing I try to fix with any injury. If the feet are strong, they can cushion the impact of gravity, alleviating pressure on the knees, hips, and back. As ballerinas know, the feet can't be strong enough! However, don't overwork them. Leave recovery time between strenuous activities.
Exercises with and without Resistance
Walk barefoot around the house and pick up marbles when you talk on the phone, do the dynaband while watching TV. Invertors and evertors pressing against the leg of a table. Resisted dorsiflexion with one foot on top of the other as you do sit-ups. Towel pulls, adding a weight on the other end for resisted intrinsic muscles.
Don’t Drown: Break it Down-Toe, Ball, Heel
1) Peel your foot off the floor, one section at a time lifting your knee and pointing the foot.
2) Lower it to the floor, toe, ball of the foot and heel.
Flexion
1) Lie on your back with your knees bent. Lift your right foot and place the band over the sole of the foot. Begin with the toes and ankle dorsiflexed.
2) As you point your foot, pull away with the band until you feel a strong resistance.
3) Slowly dorsiflex the foot back to the original position.
Extension
1) Lie down on your back with your knees bent.
2) Cross your right ankle over the top of your left thigh, placing the band over the top of the right foot.
3) Dorsiflex your toes and ankle toward the ceiling. Your left hand stays on the floor, pulling down on the band for resistance.
4) Slowly point your foot back to the original position.
Eversion and Inversion
The following helps rehab or prehab a sprained ankle.
1) Lie on your back with your knees bent.
2) Cross your right ankle over the top of your left thigh, placing the band on the outside of the right foot, holding it in the right hand.
3) Begin with the foot pointed and inverted.
4) Slowly evert the foot, pushing the little toe away from you as you pull in the opposite direction with the band. Feel the muscles working from the little toe along the outside of the shin.
5) Slowly let the foot return to the inverted position.
Do the same exercise with the foot dorsiflexed instead of pointed.
Inverters
1) Reverse the exercise by placing the band on the inside of the foot and contracting the muscles from the big toe up the inside of the shin. Do this from a dorsiflexed everted position as well as a plantar flexed everted position, always resisting the movement by pulling in the opposite direction with the band.
Metatarsal Arch
Always roll through the foot to work both the instep and the metatarsal arch in all exercises. To isolate the metatarsal arch, dorsiflex the ankle and concentrate on pointing the toes. If your toes cramp up, place your fingers between each toe to separate the digits. Then contract the metatarsal arch against the resistance of your hand. Here is the church, here is the steeple, open the doors and see all the people! Remember when you played this as a kid by interlocking your fingers. You can do a similar exercise by locking the fingers to the digits of the toes to resist flexion and extension, covering each toe with pressure from a finger. This is a great exercise if you tend to hammer your toes, crumple up and compress your toes, and if you want to focus on the metatarsal arch.

 This patient has strong muscles but relatively flat feet, while this patient has high insteps, a weak metatarsal arch, bunions, and general pain through the foot. The feet can't be strong enough!
This patient has strong muscles but relatively flat feet, while this patient has high insteps, a weak metatarsal arch, bunions, and general pain through the foot. The feet can't be strong enough!

Omni-directional Exercises
Circle your ankle, moving through all points of the dial with your toes. Write a sentence with your feet to develop flexibility. Pick up marbles or beads with your toes. Squeeze silly putty between your toes.
Calf Raises
Your body weight is your resistance as you lift your heels off the floor in a standing position.
To target different fibers of the calf muscles, do calf raises with the legs in parallel, turned in, and turned out, with the knees bent and the legs straight. Once you have the strength, do calf raises separately on each leg. Vary the tempo and the range, going up to a full releve, as high as possible. I once tore the proximal fibers of the medial gastrocnemius muscle because I didn’t do a high enough releve.
 Stretch your Achilles tendons as often as possible.
Stretch your Achilles tendons as often as possible.
Use balance board for proprioception--a BAPS board, the other end of a BOSU, or even a log
Walk on toes and heels, sideways
Ideokinesis
Think of opening up your feet to the earth, spreading your toes apart like flowers, and letting your heel dig into the earth when you stand or sit. Feel the energy of the earth moving upward through your body from your feet. When you walk let your feet be as supple as fingers. Make your feet point in the direction of your activity. If you are walking forwards, don't turn out like a ballerina; if you are jumping up in a turned out position, make sure your knees and feet are aligned. Put equal weight on all toes.
Activities
If you can't support weight-bearing, keep your feet moving while lying in bed or sitting. Aqua jogging will condition the whole body but be careful getting in and out of the pool. When you start to walk again, review gait analysis in Stride, Don't Ride, and perfect your biomechanics.
Massage
Foot reflexology is an excellent way to relax the feet, ground the earth chakra, and stimulate the nerves. Swedish and medical massage should include friction, petrissage, drainage of all muscles and tendons of the lower leg. Transverse friction of the flexor tendons distal to the medial malleoli or inner ankle bones is an effective way to release tendonitis pain from jumping, running, or pointing the feet.
Ch08: Knocked-Out Knees
Anatomy/pathology
Knee Alignment
Knock-kneed
Knock knees are sometimes called kissing knees or squinting patellae. It seems as if they are going to knock together. If you have this problem, strengthen your abductors, or outer thighs, your gluteals or buttocks, and the external rotators of your hip, so that you open your thighs enough to align your knees properly. Sometimes older women get this condition as their buttocks soft. The solution: kick butt!!
Bow-legged
Bow-legged is the opposite problem where the kneecaps point outwards in a kind of cowboy stance. Many men have this condition as a result of weakness in the inner thighs. Since there are five inner thigh muscles--adductor magnus, longus, gracilis, pectineus, and sartorius-- you must strengthen your inner thighs with the knees bent and straight. Wrestling is a great exercise as is side-lying leg lifts with resistance. Stretch your ITB, or iliotibial band.
Excessive Loaded Flexion and Compression
You can put too much weight on the knees when lifting, exceeding your compressive force potential, especially when you are flexed too much, more than 90 degrees.
Genu Recurvatum
What this means is that the knees are way too hyperextended. This can be a problem for the anterior cruciate ligament, particularly if you jump and land in this position. When you straighten the knee you want to use the vastus medialis to pull up the kneecap. You don’t want to push into the back of the knee. Strengthen your hamstrings.
Correct
Ballet dancers spend forty five minutes every day at the barre trying to perfect their knee alignment, so that the kneecaps point towards the second and third toes when they bend. However, ballet dancers may also hyperextend the knees.
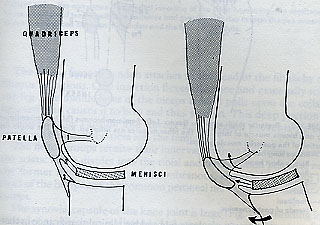
The knee has a screw-home mechanism that makes it rotate into extension and flexion, making it a modified hinge joint, with two joints, the femoropatellar and the femorotibial.
It appears to be a simple joint but a closer look at its intricate, interweaving ligaments, cartilage, tendons, and bursae over the convex and concave surfaces of the femur, patella, tibia, and fibula show that it is quite complex and vulnerable to injury especially when running, kicking, twisting, turning, jumping, bending, stooping and squatting. When the knee flexes and rotates the menisci travel forward. Then if extension is not controlled, the meniscus may not return to its normal position fast enough, getting pinched between the condyles. If a piece is torn, it may heal, it may flap around interfering with movement, and it may be necessary to remove it surgically. Please get an MRI!
You can live without menisci but they cushion the thigh bone on the shin bone, thereby mitigating wear and tear which may lead to arthritis.
Leg alignment is so important to bring your knees into a happy hab state. A lot of bow-legged and knock-kneed alignment can be corrected by training the knees to bend over the second toe, controlling the movement from the hips, lifting the insteps to avoid foot pronation, strengthening the muscles of the hips. In physical therapy therapists stress thigh strengthening but unless the feet cushion the landing and the abdominals pull up all the weight goes into the knees. On the other hand I used to ski with a 25 year old man who lost all the cartilage and ligaments in his knees and he did better than me on the moguls. While fixing the back is a delicate operation, knee therapy is a matter of strengthening, stretching and improving alignment.
Injuries and Arthritis
Pain in the Knee
Chondromalacia Patellae could be the beginning of knee arthritis or just irritation due to a wide Q-angle and a lateral quadriceps pull. When you press down on your kneecap, you may feel pain or a crunchy, creaking noise called crepitation.
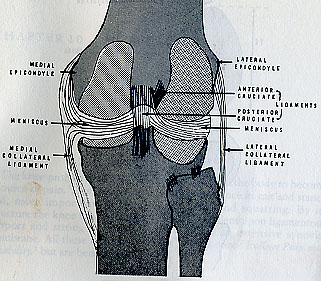
Anterior and Posterior Cruciate Problems
The cruciate ligaments crisscross and limit rotation of the tibia upon the femur. The posterior cruciate ligament prevents excessive internal rotation and flexion, while the anterior cruciate ligament prevents excessive external rotation and hyperextension. This causes anteroposterior instability, eliciting a positive drawer sign.
Meniscus Problems
Medial gets injured more than lateral-3 to 20 times more frequently. Meniscus injuries are usually caused by violation of internal rotation during flexion or external rotation during extension, usually when twisting on a weight-bearing leg. You may or may not have joint locking, swelling, and pain, depending on the degree of tear and where it is trapped. It is complicated because lateral meniscus tears can refer pain to the inside of the knee. Cysts can develop in degenerated menisci and usually occur in the lateral rather than the medial menisci. A tear in the outer third can heal unless the patient is elderly and arthritic.
A medial meniscus tear can include a tear of the medial collateral ligament, a strain of the semimembranosus, and even a cruciate tear. Sometimes just a third of the meniscus tears, which enables it to grow back to a relatively normal state in younger people.
Ligaments
Medial and Lateral collateral ligaments can be torn from a sideways stress or in a severe tear of the menisci. When this happens the joint can move into ab-adduction with the knee extended; hence the joint is unstable.
Arthritis
Knee arthritis can be degenerative or rheumatoid. You may have pain, stiffness or aching related to movement. With rheumatoid arthritis you will have redness, swelling and flare-ups with remission. These can be evaluated with radiographs and blood tests. Gentle exercise, swimming and eventually low resistance biking may help.
Bursitis
Knee bursitis can be debilitating. Your knee can swell so much you can hardly move and then you have to have it excised or aspirated. Still, aqua jogging and biking with no resistance are usually possible when more impact is difficult.
Pes Anserinus. The medial insertion of the outer hamstring, the semitendinous, forms a confjoined tendon with the sartorius and gracilis muscles to form the pes anserinus. A bursa is nestled between this tendon and the femoral condyle.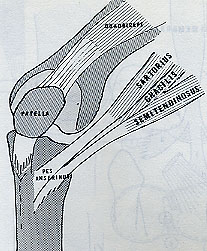
Housemaid’s Knee is bursitis from bursae located beneath the skin and between the patella and the tibial tubercle. It may be necessary to drain inflamed bursae.
Muscle Tearing of the Hamstrings
This injury can occur in bodybuilding squats when the torso is too far forward, or in extreme stretches when one of the hamstring groups is too weak--ballet penche. Good mornings and deadlifts work the hamstrings eccentrically and concentrically but be careful of these if you have a bad back.
Patellar Tracking and Quad Coordination
Knee Exercises
If you injured your anterior cruciate ligament, you should avoid the terminal extension exercises with weights and focus on hamstring curls, mini-squats, stationary biking. When you have enough muscular protection against hyperextension, begin to strengthen the quads in full range.
 Isometric quad setting
Isometric quad setting
You can do this in any position, but it is easiest just sitting on the floor with the injured leg extended. Place a small pillow or towel under the back of the knee.  Contract the quads so that the kneecap moves upwards as you straighten your leg and push your heel away from your pelvis. The whole leg should be taut and strong, but not hyperextended.
Contract the quads so that the kneecap moves upwards as you straighten your leg and push your heel away from your pelvis. The whole leg should be taut and strong, but not hyperextended.  Quad setting can and should be done in side-lying position as you strengthen the adductors
Quad setting can and should be done in side-lying position as you strengthen the adductors and in a prone-lying position to isolate the vastus medialis from the rectus femoris.
and in a prone-lying position to isolate the vastus medialis from the rectus femoris. 
As you get better, strengthen your quads in a standing position.
Stretch and strengthen quadriceps and hamstrings
Stretch your quads lying on your back with your knees bent by lifting your pelvis into a bridge.
Stretch your quads lying on your side by bringing your heel towards your buttocks and pushing your pelvis forward to target the proximal fibers of the rectus femoris.
Stretch your quads while standing by bringing your heel to your buttocks.
Hamstring Stretch: While sitting in a chair, lift your foot and straighten your knee so that your shin is parallel to your thigh. Bend over the leg with a flat back. When you strengthen your quads, you stretch your hamstrings, and vice versa. 

Don't do the Downward Dog stretch if you have a bad back. Otherwise, it is a thorough stretch for hamstrings and back.
The Chain Gang
Closed Chain Exercises
A closed chain exercise is one where the foot is in contact with the floor as in squats or lunges.
Mini-Squats
The simplest closed chain exercise is a mini-squat, or knee bend, similar to what dancers do to warm-up. This can be done with the legs completely together, with the knees hip width apart, or with the hips turned out in second position. At all times the kneecaps should bend towards the second and third toes, never flexing more than ninety degrees.
If you take this deeper and further you have a squat. In a parallel squat, always keep your weight on your heels, and the buttocks as far back as possible as if you were sitting on something behind you.
In a turned-out squat, the spine stays vertical, and the buttocks drop straight down between the legs.
Wall Sit
The simplest way to practice a squat at home on your home is with the wall sit. Stand with your back against a wall. Your feet should be shoulder width apart and about a foot from the wall. Gradually move your feet out until your legs form a right angle. Make sure you have sneakers on so you don't slide and suddenly end up on the floor. To strengthen your inner thighs as well as maintain your knee alignment, put a ball, towel, or pillow between the knees. Hold this position for as long as you can. When you start to fatigue, push your hands back into the wall, exhale and contract your abs, to help you return to standing.
One-legged Squats
The easiest way to begin this is to stand sideways on a bottom step, or the Step, holding lightly on to a railing or the wall for balance. Slowly bend the knee until the opposite foot lightly touches the floor, then slowly straighten the knee.
The key word here is slow. Bend and straighten as slowly as you can.
To do a real one-legged squat, place the foot of the leg top down on a step behind you as you bend and straighten the front knee. You may need to hold the railing lightly for balance until you can do it alone.
Lunges
From a standing position, step forward with one leg into that 90 degree position. At the same time, lower your back knee until it is 2 to 3 inches from the floor, then return to standing. It takes skill to estimate the position. Using Gliders or the Slide, you can slide into this position. Alternate legs.
Lunge backwards or forwards but do equal reps on both sides or start and end with the injured leg until you have equal strength in both legs.
Side Lunges
Step out to the side with one foot, bending the knee over the second and third toes, no more than ninety degrees. Keep your hips facing front as you lower them to the floor. Alternate legs.
As you get stronger, add weights for resistance. Eventually you will be able to get a great closed-chain cardio-strengthening workout.  Keep the knee over the heel and don't use weights like these until your rehab is over. Do lunges on the flat with no resistance, then gradually increase the height of the step and the weight.
Keep the knee over the heel and don't use weights like these until your rehab is over. Do lunges on the flat with no resistance, then gradually increase the height of the step and the weight.
Hinges
Hinges work the quads eccentrically, in their lengthened state.
Backward Hinge
1) Begin kneeling with your spine and thighs perpendicular to the floor.
2) Slowly lean backward 3 to 6 inches keeping your core muscles contracted so you neither arch nor round your back.
3) Hold for ten seconds, exhale but keep the torso stiff, and then return to starting position.
Forward Hinge
While kneeling, hook your feet under a secure object and slowly lean forward 3 to 6 inches. Again, keep your torso stable and strong, neither rounding nor arching your back. If your knees are sensitive, kneel on a well-padded carpet or mat, trying to put as much pressure as possible on the top of the shin bone, rather than squishing the center of the kneecap.
Pain
If you have housemaid's knee, chondromalacia patellae, or any kind of bursitis, do not kneel on your knees.
Open Chain Exercises
In open chain exercise the foot moves freely through space as in leg extensions, leg curls, hip adduction and adduction.
Don’t put a weight on your ankle until the joint is stable and locked. That is why open chain exercises got a bad name-they overstretched the knee ligaments and irritated the joint because of bad form.
You can do leg curls prone, in cat's cradle, sitting with a band, or standing. Dorsiflex the foot and try not to rotate the knee, just hinge it. However if the hip is turned out you will target the biceps femoris, turned in and you get the semimembranosus and semitendinosus.

Leg curls can target any of the three hamstring muscles depending on the angle. If you are turned out, the biceps femoris is the prime mover, turned in, you are initiating with the semimembranosus or semitendinosus. Ballet dancers often tear these medial hamstring muscles even though their biceps femoris is very strong. So change the angle of rotation when you do leg curls as a preventive measure.
You need it all!
You can do leg extensions lying on your back with the hip internally or externally rotated, on your side to work the ITB, in a sitting position, or standing. These are good for all knee problems except that if you have an anterior cruciate, don't use ankle weights or hyperextend the knee.
Balance Quads and Hams
Just because you can’t see the back of your thighs, doesn’t mean you shouldn’t work them as hard as the front. Biking tends to overwork the front, running can overwork the back, climbing upstairs works the back, downstairs the front. If you don’t have time, then do 12 reps for the quads, 12 reps for the hamstrings and avoid sets, rather than just doing the muscle group that was injured.
Ideokinesis
A dance teacher of mine used to tell students with knee injuries to pretend they had no knees, just feet lengthening out of the pelvis forever. This helped take the pressure and the compression off the knees. Another image is to pull up the kneecap when straightening the leg instead of pushing into the back of the knee and hyperextending it.
Activities
If you are having trouble with stairs, begin in the pool with less resistance.
Bike--stay in saddle and avoid too much resistance
Slide if no pain (some lateral training may be contraindicated for people with lateral meniscus problems)
Quad setting, straight leg raises, biking, walking, and mini-squats are usually okay for this rehab. Continue to strengthen your feet to cushion impact and stretch your hips so that all the rotation occurs there and less at your knee.
You may think you can’t do certain things like step or stair climbing or hiking because of your bad knees when in fact, some of these activities would strengthen your thighs and mitigate the pain.
Massage
Transverse friction of the entire ITB in side-lying position followed by stretching and drainage is great for a lateral release. Friction the quadriceps tendons to help mobilize the kneecap.
Ch09: Creaky, Crackling Hips
Anatomy/pathology
The six rotators of the hip, (gemelli inferior and superior, internal and external obturators, the quadrate, and the piriformis,) the three buttock muscles, the quads and the hamstrings all influence the movement of the hip joint. 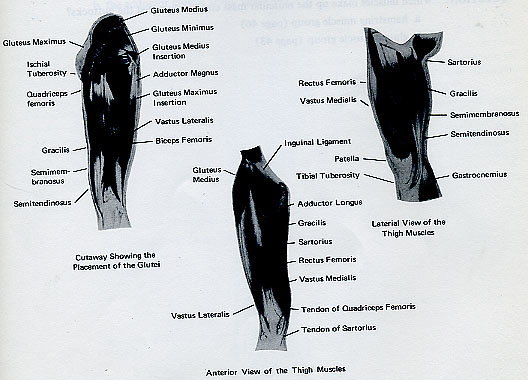
Alignment
Hips and shoulders are rotatory joints, just like a ball in a socket. If you use them like hinge joints, eventually there will be problems.
Coxa Vara: When the neck of the femur is almost horizontal with a well-developed superior rim of the acetabulum) abduction can be limited as the thighbone butts up against the bony acetabulum. If you keep banging it, excessive growth or spurs could form, further limiting your motion. As with everything else, work within your limitations.
Coxa Valgus: When the neck of the femur is close to vertical with an undeveloped superior acetabular rim, you can abduct easily.
Some ballerinas look like they are made of hot butter. Stretch to your limit, relax to exceed it, but don't force yourself into painful splits.
Are you twisted backwards or forwards? Anteversion versus Retroversion
…it-is
Arthritis
Bursitis
Tendonitis
Injuries
Piriformis Entrapment Syndrome
Iliopsoas Imbalance
Pain in the hip can come from the capsule and its ligaments, the surrounding muscles, the bony periosteum, or the synovial lining of the joint. Aside from direct trauma and dislocation, the most painful hip condition is degenerative osteoarthritis.
Exercises for Muscle Balance
Piriformis syndrome can be caused by weak, bruised or overworked buttocks.
Rotator exercises
Side lying rotation
Lie on your side with your knees bent at 90 degrees and your hips stacked.
Turn your hip out so that your top knee points to the ceiling.
Do not move your pelvis.
Then turn your hip in so that your knees touch and your feet are separated.
Turn thighs in and out in other positions such as back-lying, supine and standing.
Abduction
For therapeutic purposes, begin your sequence with isometric buttocks contractions, pushing your legs against something in back-lying position.
Keep your legs straight in side-lying position.
Lift your top leg with the heel pointing towards the ceiling and the toes to the floor.
Level III can bring the top leg forward at a 90 degree angle and continue abduction in this position.
Keep the pelvis still by contracting the abs.
Then do leg lifts with the hip turned out, heel towards the floor and toes to the ceiling. Again, don’t move the pelvis
Gluteus medius and minimus lift leg to the side--medius is targeted with slight external rotation and abduction; minimus with internal rotation and abduction.
Then standing side lifts.
Bands
Pulley machines are great but you can attach your band to table leg, to doorknob, to upper door hinge for the same kind of movement. Add bands to weights for more resistance. Bands can snap and they don’t develop fast twitch power at the release because they recoil back. Their recoil can be so strong that you lose all eccentric muscle training. So work slowly and use weights as well as you get stronger.
Adduction
Squeeze a ball, pillow or thigh squeezer between the knees for isometric contractions.
Lie on your side and lift your underneath leg up and down. Bend the top knee and put it on a pillow.
Straighten the underneath leg and move it up and down, changing the rhythm and the angle.
Target the parallel fibers with the other knee in front.
Then turn out and open up the top leg to target the turn-out inner thigh muscles. To target different adductors, turn out the top leg and bring it behind the underneath leg. Push the pelvis forward and contract the buttocks to maintain a neutral pelvis. 
Adductors can be worked side-lying by putting the top leg on a chair to squeeze the inner thighs isometrically while the lower leg lifts and lowers.
In a standing position, use a dynaband to cross the midline as if you were slowing pushing a ball.
Do second position ballet plies, focusing on the inner thigh squeeze as you straighten your legs.
Extension
Pelvic Tilt
Lie on your back with your knees bent, feet flat. Contract your buttocks to lift your pelvis off the floor, vertebra by vertebra. Roll up and down.
Bridge
Lift one leg straight to the ceiling and keep it there as you perform the bridge with the other buttock.
When you bridge you are extending the hip by flexing your spine first. If you bridge from a bench or ball you work the hamstrings and calves more intensely.
Make sure you work both sides of the spine equally and always do the same number of reps on both legs.
Prone extensions
Lie over your step, a small table or low chair or bench so that your knees remain on the floor. Relax your back but contract your buttocks to lift your thigh off the floor. 
Do variations with bent and straight legs.
Vary the angle of rotation to target the gluteus maximus, minimus, and medius.
Standing extensions
Standing on one leg, lift the other leg behind you contracting your buttocks. You get a double whammy here because the gluteus medius of the standing leg must work to keep your balance.
However if you have leg length discrepancy or hip arthritis you may want to do this in a pool.
Dancers can put floaties on the ankles to extend their range of motion in arabesque.
Pain
If you feel pain in your back while doing extensions contract your abs strongly and don't lift the leg so high.
Flexion
Lie on your back. Bend one knee and put the foot flat on the floor.  Straighten the other leg and lift it up and down, keeping the pelvis on the floor.
Straighten the other leg and lift it up and down, keeping the pelvis on the floor.
Contract your abdominals to stabilize your pelvis.
Change the angle from turned in to turned out to get different muscle fibers.
Then do front knee and then leg lifts in a standing position.
Cat's cradle and donkey kicks
On all fours lift your leg up and down with the knee bent and then straight, turned in and turned out. If you have no injuries and want to try abduction in this position make sure your abs are tight, both arms are straight, and your pelvis doesn't move. Combining hip extension with abduction on all fours in rapid moves is good preparation for kickboxing, but only for Level III.
Try a slow balance of opposite arm and leg to activate the core muscles.
Correct gait for unequal leg length. Adjust sacroiliac. When I ran a back school for an osteopath, unequal leg length was a big problem, particularly with athletes who didn’t want to wear heel lifts during dance or sports. Over the years, it can lead to shearing stress, sacroiliac problems, herniated discs, hip and knee arthritis.
The problem with the hips (and the shoulders) is that we often think of them as mounds of flesh coming out of our torso instead of ball and socket joints. Much arthritis and injury could be avoided if we always strengthened and stretched the tiny rotator muscles that move our hips and shoulders.
Once you begin working the bigger muscles of the arms, incorporate rotation into exercises for the deltoids and trapezius.
Sequences
Stretch piriformis, iliopsoas, ITB, adductors, rectus femoris
Strengthen 6 rotators of the hip
Strengthen gluteals
Strengthen ab-adduction
Strengthen rectus femoris
Correct leg length discrepancy
Ideokinesis
Keep imagining your hips joints as oily rotary joints that can turn in and out equally and smoothly. Your spine can be separated from your hips although they are joined by the iliopsoas and piriformis muscles.
Activities
The best aerobic activity for people with hip problems is aqua jogging. Aqua jogging forwards, backwards, sideways, turn in and out. Check your leg length when you return to normal walking. Cross-train as you begin activities like ballet or sports.
For years, I treated the hips of former ballerinas. At first I signed on to the popular idea that “ballet is bad for the body.” I have changed my mind. It is okay to turn out as long as you also turn in, as long as you balance the rotators of the hip, don’t overtrain the way most professional dancers do, and avoid dancing with pointe shoes, unless you are paid to. Turn in and out equally, abduct and adduct, flex and extend. Balance the ball in the socket.
Massage
Deep friction massage of the piriformis and other rotators are essential to restoring hip function. Do this side-lying and prone.
Ch10: Low Back
Anatomy/pathology
The Hell of Back Pain
You just spent the weekend hiking up and down mountains. It's Monday morning and you can't get out of bed because your back hurts so much. Or-you lifted too much weight at the gym, pulled a muscle and now you're afraid of turning to mush. Or-you sit 12 hours a day fulfilling the demands of your company. You have just been rewarded with a raise and have bought a new home but you dread moving because your back hurts so much. The problem is that you sit crumpled and twisted all day so when you bring this dilapidated structure to the gym, it’s like laying bricks on the leaning Tower of Pisa!
Back pain, with its herniated and bulging discs and facet impingements, can be the beginning of cartilaginous degeneration and consequently osteoarthritis, so it's important to fix it before it misaligns the entire body and causes arthritis in knees and hips as well.
Over the past 25 years, I have had a 98% cure rate with back pain. I worked for a neurosurgeon and ran a back school for an osteopath for a few years, but my most dramatic results have been achieved with house calls where I analyze the patient's home or office environment and their emotional state as carefully as his/her body. If you spend hours crumpled up in a soft chair or sofa reading or watching TV, if you sleep in a position that exacerbates their particular problem, if you are angry about their work or love life, then no amount of exercise therapy and massage will fix the back for good. I watch them lie down, stand, sit, and walk through every room in their apartment. Then I copy what they do, exaggerating what they do wrong, so they have a visual image of the misalignment; and then we work to correct it. As they work on posture, they develop the kinesthesia to feel the necessary improvements themselves. Examine your furniture and check your posture with a mirror, against a wall, or through internal kinesthetic awareness. Little things make a huge difference. I had a client with severe sciatica who bought an expensive mesh chair for her office, but put the lumbar roll a few inches too low, so that it rounded her lower back, and compressed her sacrum, exacerbating the sciatica. Simply by fixing the placement of the lumbar roll, massaging her sciatic dermatome, and giving her corrective exercises, she was able to cure herself of her symptoms.
I am not a psychiatrist so I don't try to resolve their personal problems but I make patients aware of how these problems could be affecting their pain. Recently I arrived at a patient's apartment to find him bent in two with back pain. He whined: "My back is killing me; my mother just died; and the IRS is going to audit me!" I told him I would relieve the back pain with massage and exercise, but it was up to him to accept, ventilate and try to solve the other two problems so that he didn't turn them into three problems again.
When I go to patients’ homes to help them with their backs, I first look at their posture when they open the door. Then I examine the medical report, history and x-rays. After that, I look at how they walk and stand, how and where they do their chores in the kitchen and bathroom, how they sit at the table or in their favorite chair, how they sleep, and even discuss the mechanics of their sex life. If someone does the correct exercises but sleeps crumpled up on four pillows, or sinks into a chair with their legs crossed or walks with a limp, then these issues must be addressed even before we work on the exercise program.
My approach to exercise focuses on subtle variations for individual differences, constant attention to posture and movement quality, working muscles that most classes and gyms leave out, incorporating balance and coordination with the other fitness components of strength, flexibility and endurance, cross-training, and really developing one's physical potential as carefully as an educator develops one's mental potential.
Low back pain can be caused by a strain, a sprain, a spasms, injury, arthritis, or just weakness, and bad posture.
Alignment/Posture
Posture is simply the way the parts of your body are aligned in terms of the forces of gravity. Just as a building must have a solid foundation, so should your posture be something that conforms to the optimal alignment for gravity and the structure of your joints.
A normal spine has four natural curves balanced over a plumb line but exaggerations can form a C-shape in kyphosis, a U-shape in lordosis, or an S-shape in scoliosis.
Scoliosis
The S-curve can cause back pain and even the conditions that for a herniated disc. You can have congenital scoliosis from birth, traumatic scoliosis from an accident or partial paralysis, or degenerative or insidious scoliosis from muscle imbalances and arthritis. We all have a little scoliosis caused by our handedness, slightly unequal leg lengths and postural quirks. When scoliosis becomes severe, it can damage discs and contribute to facet impingements and the formation of osteophytes.
Performance
Use a light effort to move your arms and legs but to strengthen your abs, use a strong exhalation that really deflates the balloon in your pelvis.
Scoliosis is corrected or mitigated by always working both sides equally on all exercises and class sequences. Lift equal weight on each limb and try to use your weaker hand as much as possible. Correct yourself visually and kinesthetically. Be careful of sports like tennis that favor one arm and one side. Practice with your weaker side and make sure your weaker arm can always lift as much weight as your stronger arm. Do lots of rows and pull-downs to keep both sides of the back equally strong.
Kyphosis
There should be a natural kyphosis in the thoracic and sacral spines. However many people develop excessive kyphosis in the middle spine from round shoulders, forward head and weak back muscles. In extreme cases, this can lead to respiratory problems as well as back pain.
All the curves affect each other so that a person with excessive lordosis in the lower back might have too much kyphosis in the middle back.
To correct kyphosis, stretch your chest muscles, strengthen your middle and lower trapezius, rhomboids and lats. Imagine a huge diamond necklace shining on your chest.
Lordosis
Some lordosis is necessary in the cervical and lumbar spines to create good alignment, but excessive curvature can pinch facets or lead to stress fractures or other problems.
Lordosis is corrected by strengthening the flexors such as the abdominal muscles, by strengthening the spinal extensors eccentrically in their lengthened state, by stretching the lower back and neck, by correcting neck and pelvic alignment, and by stretching the hip flexors such as the iliopsoas. If the lordosis is severe in the lower back, you may have to strengthen the lower buttocks in posterior pelvic tilt to neutralize the pelvis
Inappropriate spinal curves may or may not be painful. Try to correct them anyway.
Balance the Bowl: Pelvic Alignment
Posterior Tilt
In a posterior pelvic tilt, your pubic bone is ahead of your top brim of your pelvis, the anterior superior iliac spine, in the vertical line of gravity.
Anterior Tilt
In an anterior pelvic tilt, your pubic bone lies behind the anterior superior iliac spine, in the line of gravity.
Neutral Pelvis
In a neutral pelvic, no water spills from the bowl. In other words, your pubic bone is on the same vertical plane as the top of the basin.
Tipped Pelvis
Your pelvis could also be tipped to one side, a condition that often occurs with unequal leg length.
Sitting
Sit on your sit bones, the tuberosities of the ischia, not your tail bone. Rock back and forth until you feel equal weight on each side. Put your feet flat on the floor. If you can't reach, put them on telephone books or lower the seat of your chair. On the other hand if the angle between your torso and thighs is greater than ninety degrees then raise your chair seat.
It is hard to keep your chest lifted when working or eating but keep pressing your shoulders down and imagining eyes in the back of your head.
Standing
Do the wall check. Place the back of your head, your shoulders, buttocks and heels against the wall. There should be a natural hollow for your lower back. Contract your abdominals without flattening this arch.
Wall Check
(Lateral view)
Posture: If you are obese or pregnant, the wall check won't work so just work on your plumb line from the side.
Walking
Take this standing posture into a walk as if you have headlights on your collar bones and your head is the tip of an iceberg coming out of water.
Imagine your arms swinging naturally like pieces of silk in the breeze.
Sleeping
Yes, it is possible to sleep incorrectly, contorted into positions that strain your muscles and damage your discs. Sleep on your side with a pillow under your head but do not curl into a foetal position. Sleep on your back with lumbar and cervical rolls. Only use pillows under your head if you have respiratory problems. It would be better to have a gradually sloping medical bed than to flex your neck too much.
Lifting and Bending
Always remember to bend your knees and keep your back straight when lifting.
Common mistakes while lifting and bending are:
Inadequate warm-up for lifting
Not enough strength for the load
Feet too close together
Lifting too far from the body
Unbalanced load
Too much repetition without rest
When you have back pain, don't be a kinesophobe. Use it or lose it applies to your back as well, but just be careful. Always bend your knees and lift with your legs and arms, keeping your back as long and arched as possible although you should exhale and contract your abs as well. Don't curl your back to straighten, especially with heavy loads. Some say tuck under, others say keep your back straight. I say use your core muscles and try to move the back as little as possible, using the arms and legs to do the work. Get your center of gravity beside your load.
When cleaning, make sure you are stable on your ladder. Keep your back aligned and work from your lats.
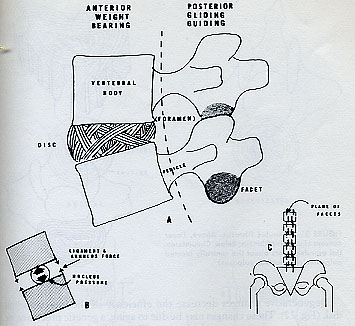
Discs: Healthy and Degenerated
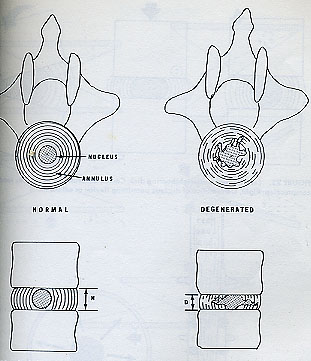
A herniated disc can also be called a slipped disc. A healthy disc is like a grape wedged in between your vertebrae. Under pressure it can bulge out, occasionally pinching a nerve. It can also slip or herniate in such a way that its fragments pinch a nerve. Once the grape is gone, the vertebral bodies have no cushion between them. It is easier for the facets to pinch together or posterior osteophytes to form, a kind of back arthritis. As we get older, the nucleus pulposus, or grape, gradually dries up and turns into a raisin.
The most common areas for herniation are L4-5 and L5-S1, but you can also herniate L3, either from trauma or because the low back develops a kyphotic rather than a lordotic curve.
The most troublesome symptom of a herniated disc is pain running down the leg from the buttocks.
You may have disc problems without even knowing it. If your radiographs show a herniated disc and you have radiating pain down your leg, you should follow a strict program of back exercise, refrain from violent sports, and get your aerobic exercise walking or aqua jogging until the disc is stable, the pain is gone. If you have the skill to isolate your back muscles, you can do weight lifting for arms and legs.
If you have a foot drop, numbness or weakness in the toes, see a doctor immediately.
Radiculopathy is radiating pain from the nerve impingement. Don't twist the spine in an effort to get rid of this pain. I have seen people twist their arms and legs in knots to massages themselves, putting their backs in contorted positions and making the impingement worse.
Pain can travel from back to buttocks to posterior thigh to lower leg, weakening the quadriceps, buttocks, calves and big toe extensors, causing a tingling sensation in the toes or heel.
Neck pain can radiate down the arm to the fingers, in between the shoulder blades, in and around the neck, ears and face.
Facet Impingements and Osteophytes
The reason discs herniate more frequently in the low back is because the posterior longitudinal ligament covers only about fifty percent of the disc space there. Although the discs will dry up, aging doesn’t have to cause disc disease. Shearing stress can cause disc rupture, particularly at L4-5 and L5-Sl in the low back and C5-6 and C6-7 in the neck. Your upright posture imposes a compression stress on discs as you fight gravity but this doesn't have to cause problems if your alignment is good. However as the grapes burst out or dry up into raisins, the vertebral bodies get closer together, the facets rub together creating bony spurs called posterior osteophytes. In this case there is less ability to hyperextend the spine.
Facet impingements and osteophytes require a traction or lengthening approach to exercise. Don’t do anything to compress the spine. Sometimes facet impingements can unhook naturally.
If a facet impingement is stuck in flexion, it is open, in extension, it is closed. Facet impingements are best treated with Water therapy, medical massage and mobilization rather than high velocity chiropractic adjustments.
Spondylolisthesis, Stress Fractures and Subluxations
Congenital spondylosis is a fusion. When it fractures, it is called spondylolisthesis.
Spondylolisthesis is a condition of forward subluxation or slippage of the body of one vertebra on the vertebra below it, occurring most frequently at L5 over the sacrum in 70 percent of the cases. It can also occur at L4, 25%, or higher levels in traumatic cases or diseases. It is usually preceded by spondylolysis, a bony defect of the neural arch, which may not cause any symptoms, except if it breaks off to cause the forward slippage of spondylolisthesis. When this occurs, do not hyperextend your spine. Strengthen your back muscles toextension but don't try to arch way back.
Spondylolysis can be congenital or caused by excessive hyperextension with impact in gymnastics, competitive sports or accidents. Professional athletes are more prone to this condition than the general population but now with the emphasis on core training, the percentage of fractures is going down.
Spondylolisthesis occurs when the pars interarticularis begins to separate at the stress fractures so that the vertebral body slides forward in a forward subluxation. If you have either of these conditions, control the range of motion of extension and avoid hyperextension of the spine.
If you have Spondylolysis, Spondylosis and/or Spondylothesis, avoid anterior pelvic tilt and hyperextension.
Spinal Stenosis, TMJ, and Tumors
Spinal stenosis is a too tight canal, which you can have at birth or develop in old age. Avoid heat treatments and excessive range of motion but do simple back exercises, walking, swimming, biking.
TMJ or temporomandibular syndrome, a jaw-tightening, teeth-grinding habit, can cause neck pain and even general back pain. I remember treating a lawyer and an opera singer with TMJ by massaging the face, head and neck and doing back exercises. When we finished, the opera singer sang so melodiously she became a colaratura, and the lawyer so relaxed she gave up her practice and got married.
Always get an MRI because intraspinal tumors could mimic herniated discs from the outside. When I worked for a neurosurgeon I was privy to all the tumors, distortions and creative ways nature, gravity and you can cause back pain. So find out what is wrong, follow your PT and then continue to improve with Dr. Keefer's Corrective Clinic.
Muscle Strains and Sprains
Extensor Strains
If your back muscles are weak, and you spend the day lifting you can have a muscle strain. Hopefully this will be just a muscle strain without ligamentous or nerve involvement. It can heal like other strains with ice, rest, massage and gradual strengthening.
Ligamentous Sprains
A ligamentous sprain of the back is more serious, particularly if it leads to disc herniation, facet instability or something that might impinge the nerves. Here you must keep your structure as stable as possible to avoid exacerbation of the problem.
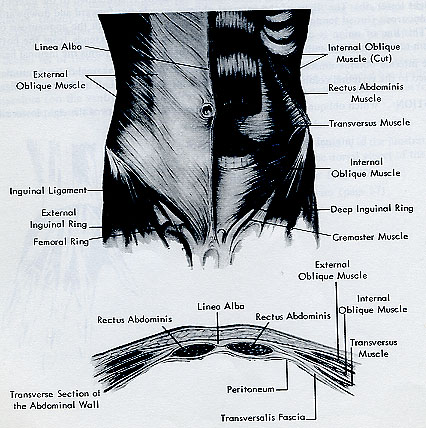
Abdominal Hernias
A hernia is a rupture in the abdominal wall, which can cause the intestines to stick out. After a hernia operation your doctor may say not to do sit-ups. The irony is that it is the best way to correct and prevent hernias is by strengthening the transversus abdominis so it acts as a tightly knit band of fibers protecting the intestines.
There is a difference between the low back program and the neck program, although they are related.
Low Back Protocol
Establish a neutral pelvis by strengthening your transversus and multifidus muscles. To simplify this, let me talk about balloons.
Inflate the Balloon
Inhale and let the ribs expand sideways like a fire bellows. Let the belly swell a bit just so you can deflate it with your exhalation and breathe mainly from your diaphragm.
As you exhale, deflate the balloon in your abdomen by contracting your transversus abdominis and internal obliques.
One of the most important muscles in the body is the transversus abdominis, which not only help to give you a flat stomach, but stimulates your internal organs, guards against hernias, facilitates urination and defecation, and aids in reproductive and sexual activities. Place a rolled up towel at back of belly button. Exhale, deflate a balloon and press the navel into the back, not the back into the floor. Or put a blood pressure cuff inflated to 40 mmHg. If the pressure rises you have gone into posterior pelvic tilt; if it lowers drastically anterior. Only expect a 3-5 degree change.
Multifidus are deep and associated with pelvic floor or stopping the flow of urination-in men as well? These muscles come first. They are the impulse for everything.
The Squeeze (that’s Aimed to Please)
The deep core muscles are connected to the pelvic floor muscles inside the vagina and anus. Good tonus here is essential for sexual and reproductive activities as well as helping to maintain a neutral pelvis and efficient abdominal organs.
Important Back Stretches
Stretch in cat's cradle
Get on all fours on a carpet, bed or mat with your hips you’re your knees and your shoulders over your hands. Visualize your back as a tabletop. Exhale and round your back, turning it into the letter C. 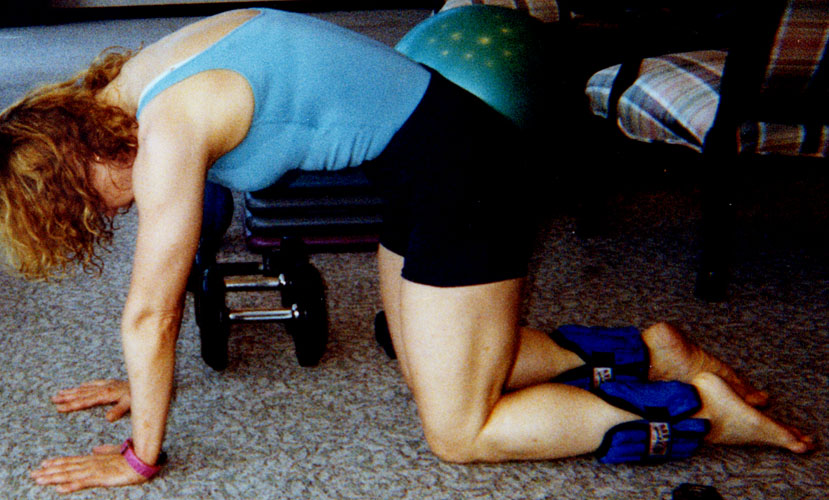 Then inhale and arch your back, making the letter U.
Then inhale and arch your back, making the letter U. 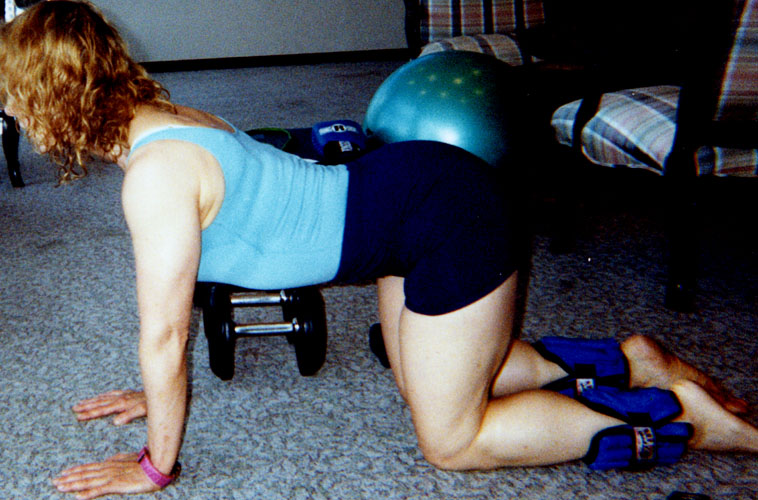 Don’t move so much it hurts, particularly if you have a disc problem. From this cat's cradle position you can do some safe lateral bending and
Don’t move so much it hurts, particularly if you have a disc problem. From this cat's cradle position you can do some safe lateral bending and rotation with dog wags and thread the needle.
rotation with dog wags and thread the needle.
Iliopsoas

This is best done lying on your back on a hard surface with your buttocks at the edge of a table. Bring one knee you’re your chest and hold it there, as you let the other leg dangle off the table. Don’t twist or arch your back.

Also in side-lying let thighs fall off the table. Inflares and outflares produce groin pain. Shock absorbers, stabilizers, accelerators and decelerators.
Hamstrings
Hamstrings can be stretched in many positions but make sure you don’t round your back at the same time.
It is important to have enough hamstring and low back flexibility to actually get into the arched back lifting position.
1) While sitting in a chair, lift your ankle and straighten your leg until you feel a stretch behind the knee.
2) In a standing position, bend your left knee and place it behind the right leg. Straighten your right leg and dorsiflex the ankle. Arch your back and lean over slightly. Be careful not to round your back, especially if you have a disc problem.
3) Lie on your back with a rolled up towel under the back behind the bellybutton. Straighten one leg and put the band around the ankle. Keeping the leg straight, gradually pull it towards you.
This, coupled with a dorsiflexed foot and neck flexion, is one of the tests for sciatica so don’t round your back or lift your leg too high.
Piriformis
Sit in a chair on your sit bones, not your tailbone. Cross your right ankle over the top of your left thigh. Arch your back and bend towards the right foot, keeping both sit bones on the chair. Use pressure on your right knee if necessary. Do the piriformis stretch anywhere, everywhere to avoid piriformis syndrome as well as to stretch the sciatic nerves.
Do the piriformis stretch anywhere, everywhere to avoid piriformis syndrome as well as to stretch the sciatic nerves.
Start with isometric abs, then quarter-ups, then sit-ups. Never pull on your neck, exhale on the exertion and flatten your abdominal wall so that the hip flexors don't take over and pull unevenly on your spine.
Half sit-ups
Extensor exercises
Lie on your stomach with your forehead on the floor for a few seconds.
Then prop yourself up with your forearms in the Sphinx position.
Allow your back to relax into a lumbar curve.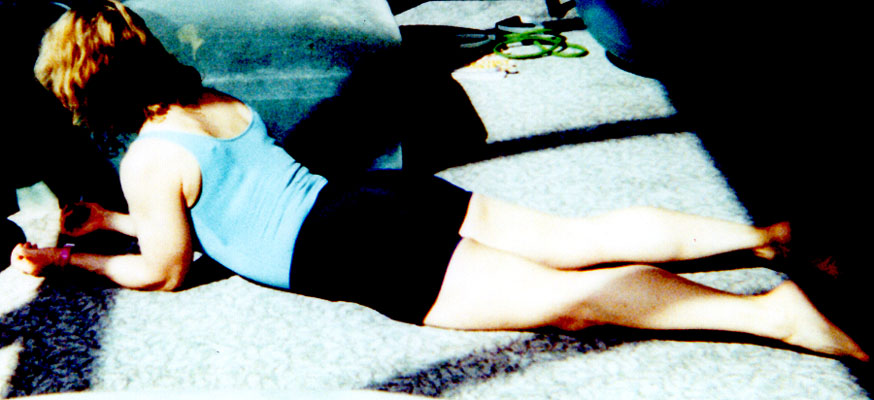 Only Level III should come all the way up into the Cobra--it is usually too much for Levels I and II or people with spondylolisthesis, stress fractures, or posterior osteophytes.
Only Level III should come all the way up into the Cobra--it is usually too much for Levels I and II or people with spondylolisthesis, stress fractures, or posterior osteophytes. 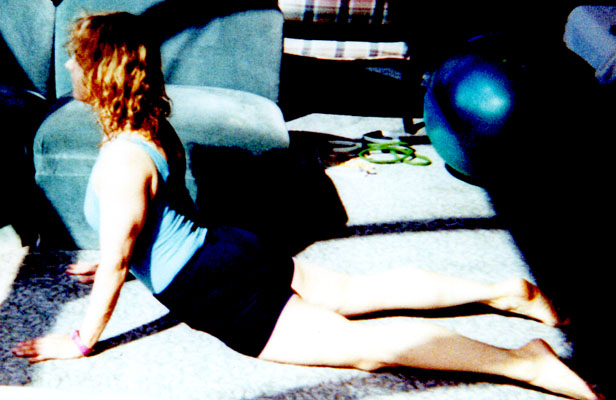
Lace your fingers together behind your head and lift your neck off the floor. Hold for ten seconds and lower.
Keeping your forehead on the floor, lift your opposite arm and leg off the floor. Keep the leg low. Then lift both together in a taffy pull, as long as you don't have spondylolisthesis or posterior osteophytes. 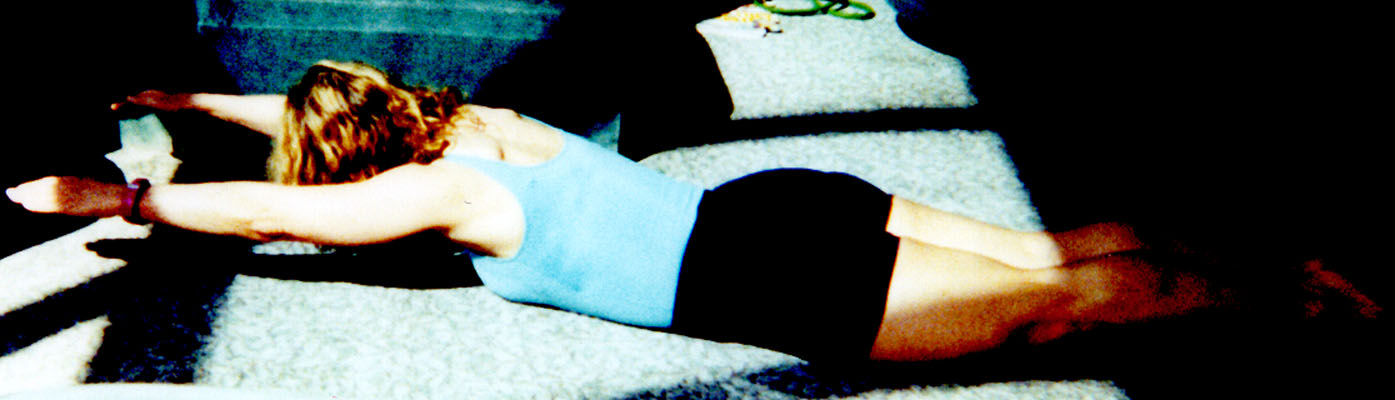
Lace your fingers together with your arms straight and lift your chest off the floor.
If you cannot do hyperextension, lie prone on a table with your feet held by someone or hooked into something secure. Let your torso hang off the end of the table towards the floor. Slowly lift your torso in one movement until it is parallel with the rest of your body. This exercise allows you to contract the back muscles without hyperextending the spine.
 This patient has severe kyphosis in her family but has managed to avoid it herself, even though she is seventy.
This patient has severe kyphosis in her family but has managed to avoid it herself, even though she is seventy.  Her secret? Back extension exercises!
Her secret? Back extension exercises! 
Isolate arms from core
Isolate legs from core
Work arms and legs against core to stabilize spine.

Here is one way I fix backs, especially when doing house calls.
A.You should learn to do your own postural assessment in a standing position.
1) Do you have a neutral pelvis or an anterior or posterior pelvic tilt? Where is the pubic bone in vertical relationship to the ilia?
2) Is your lower back too arched or too flat?
3) Is your upper back too rounded in a thoracic kyphosis?
4) Do you have a forward head with your ears ahead of your shoulders?
5)
Symmetry:
Do you have equal weight and support on both legs, equal ilia height, equal leg length, equal shoulder height, no lateral or rotary rib cage shift?
B. Corrective Stretches (Stretch both sides equally)
1) Iliopsoas off table or bed
2) Hamstring stretches in chair, runner's stretch or on table or bed. (Very tight hamstrings can cause posterior pelvic tilt.)
3) Piriformis stretch supine or sitting.
C. Constructive Rest
Lie in a non-weight bearing position for several minutes to relieve excess muscle tension and stress. If you have a back strain, an anterior pelvic tilt or spondylolisthesis, you may want to bend knees and relax in supine. If you have a disc and a flat back, and have been sitting a long time, rest in TV watching or sphinx position, then make sure you have a lumbar roll in supine. Use ideokinesis to relax all muscles and deepen breathing.
D. Quadruped series --(Limit ROM if you have a disc)
1) On all fours contract and arch spine.
2) Dog wags for quadratus lumborum
3) Thread the needle for rotation
4) Opposite arm and leg for core stability
E. Supine
1) Transversus Abdominis versus Multifidus and pelvic floor for back stability.
2) Transversus Abdominis versus hip flexors to move legs against a stable core. Thigh flexions, single and double, then straight leg raises. If the disc is active be careful of straight leg raises. Don't let pelvis move. Open and close knees for adduction/abduction or internal/external rotation. Keep core stable.
3) Transversus Abdominis versus Latissiumus Dorsi and other back muscles to move arms against a stable core
4) Flexion: Transversus Abdominis with Rectus Abdominis, first quarter-ups, then half sit-ups. Advanced will eventually proceed to full sit-ups when pain free. Eccentric and concentric action. Different speeds.
5) External and internal oblique muscles. Add a twist isolating rib cage from pelvis.
6) Spinal twist first relaxed, then with knees together off floor.
7) More extreme oblique twists.
8) Lateral half sit-ups
9) Pelvic tilt into bridge into wheel for advanced participants with no disc problem
F. Side-Lying
1) Hips. This is especially important for people with sciatica. Turn hip in and out to stretch and strengthen piriformis. Abduction/adduction leg lifts.
Begin with the most affected leg, and do LRL, for example. See hip section.
2) Side planks with knees and arms bent and straight. Add leg lifts and rotation for advanced participants. Don't do this until your core is stable.
G.Prone
If participant is obese, has extreme anterior pelvic tilt, or spondylolisthesis, do all prone exercises off a bench or table to avoid pinching the back, isolating the arms and legs.
1) Extension series: hands behind head, hands behind neck, arms straight behind back, arms straight out in front. Leg lifts single or double. Those with an overly arched lower back should do an abdominal contraction and keep legs long and low. Those with flat back and no serious disc, lift legs as high as possible to strengthen lower back.
2) Planks, progressing from knees bent to legs straight and moving, one arm lifted etc.
H. Standing
1) Check alignment against wall
2) Neck isometrics and resisted motion in all directions. Avoid pinching discs by letting head fall back guillotine-style.
3) Shoulder shrugs and Lat pulldowns
4) Scapular retraction
5) Overhead reach
6) Rib cage shifts and circles horizontal and vertical
7) Pectoral stretches and Ys
8) Transversus Abdominis activation in standing position
9) Pelvic circles
10) Wall squats, then squats in and out of a chair
11) Lunges to pick things up
12) Calf raises and stretches. Focus on LRL for affected leg in sciatica.
13) Hamstring curls. Leg extensions. Don't go too high, depending on pathology. Focus on LRL for affected leg in sciatica.
14) Balances to strengthen gluteus medius, especially in affected sciatic leg.
15) Gait analysis. If you have sciatica, try to walk properly, because by limping, you make the condition worse.
Chair exercises should be done throughout the day at work, but once you get home give your back a break to re-establish good alignment. Too much sitting compresses the discs.
In back injuries begin with stabilization against arms and legs before spinal flexion-i.e. no situps right away. Don't do Lateral and Rotational core exercises until you have been pain-free for a while on simple flexion/extension. Supine and all fours. Straight leg supine trunk curls are also good. Essentially Level III can do anything they are capable of doing that doesn’t hurt. Once you are better, go to Knockout Cardio-Core for advanced work.
Posture affects back pain more than any other pain. It may be easier to slouch and slump but it won’t improve your pain in the long run.
For mild to moderate disc problems, just do: Isometric abs in all positions. Simple half sit-ups or quarter-ups. TV watching position. Back extension-carefully. Psoas, hamstring, quad and piriformis stretches. Postural awareness at all times. Aqua jogging. Walking if leg length is equal. Isometric wall squats. Don’t add rotation until spine is healed.
If you are very coordinated and can isolate torso from limbs, stabilizing core, you can and should continue to strengthen your arms and legs with activities you did before.
Bent-over rows, Good Mornings, and deadlifts, body building exercises usually used to strengthen the back muscles, are not ideal when your back is out. It is important to have enough hamstring and low back flexibility to actually get into the arched back lifting position.
Joint, neurologic and connective tissue limitations of stretching are important.
Lat pulldowns in correct alignment with a band from above are okay but the other exercises demand a strong, healthy back to start. Wait till you are feeling better before engaging in this type of exercise that is so demanding. Or use a step to stabilize your back while you work these exercises.
As your arms and legs swing through space, it becomes harder to keep your torso still. To do this you must contract all those muscles we’ve been talking about-gut, butt and back.
Arm movements: You want to be able to move your arms in all directions without moving your back, keeping your pelvis neutral and your core muscles contracted.
Thigh flexions: You also want to be able to move your thighs without shifting your pelvis around, which means you must have strong abdominal and back muscles.
Spinal Twist: Don’t do this if you have a severely herniated disc with active sciatica down the leg. Lie on your right side with your knees bent. Placing your right hand on your left thigh, left your left arm arc to the other side so that your left shoulder is on the floor and you are lying on your back in a spinal twist. with your arms extended at shoulder level. Let your legs move to the right keeping your shoulders on the floor, and your head in the opposite direction.
BED PROGRAM
The following are exercises you can do in bed to mobilize your back on a daily basis. Use minimal energy, breathe, relax and never push. Bring your knees into your chest to stretch your back muscles. 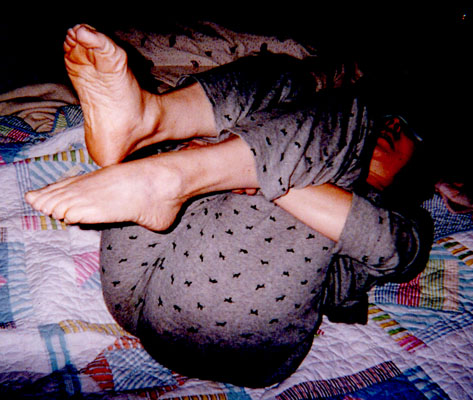 Rotate side to side.
Rotate side to side.  To keep your pelvis aligned and deep muscles contracting, squeeze a pillow between the knees before exhaling into a half sit-up.
To keep your pelvis aligned and deep muscles contracting, squeeze a pillow between the knees before exhaling into a half sit-up. 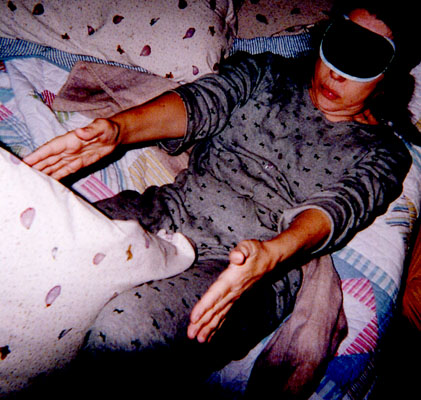 The TV watching is a great way to undo the ill effects of prolonged sitting.
The TV watching is a great way to undo the ill effects of prolonged sitting. 
 Hold the hamstring stretch for 30 seconds on each leg.
Hold the hamstring stretch for 30 seconds on each leg. 
Stretch the inner thighs keeping the abs contracted to protect the back.
Stretch the hip flexors and quads in the bridge. Stretch the piriformis muscles by crossing the ankle over the opposite leg. You can do oblique half sit-ups in this position as well.
Stretch the piriformis muscles by crossing the ankle over the opposite leg. You can do oblique half sit-ups in this position as well.
 Then relax completely for a long night's sleep.
Then relax completely for a long night's sleep. 
When you feel comfortable and healthy enough to relax over the Swiss ball, then come to Aerobic-Gut-and-Butt for some serious core conditioning.
Ideokinesis
Get into a constructive rest position and use imagery to lengthen and balance all spinal muscles. This may be lying on your back with a lumbar and cervical pillow, or lying on your side, without curling into a foetal position. It depends on the structure of your spine and your pathology.
Activities
Aqua jogging relieves compression on the discs and promotes circulation for healing.
Walking in good alignment. Use a heel lift if you have significant leg length discrepancy.
Intellectual activities are difficult if your back hurts. Watch your posture, do the daily exercises, aqua jog, and walk and you will be rewarded with a body that doesn't sabotage your mental growth and development.
Massage
Any back massage feels great but if you have a piriformis syndrome, transverse friction all the fibers from the sacrum through the sciatic notch to the hip joint and then down the outside and back of the leg. You can do this in both side-lying and prone positions.
Ready for the Upper Body? Proceed to Dr. Keefer's Corrective Clinic Part II