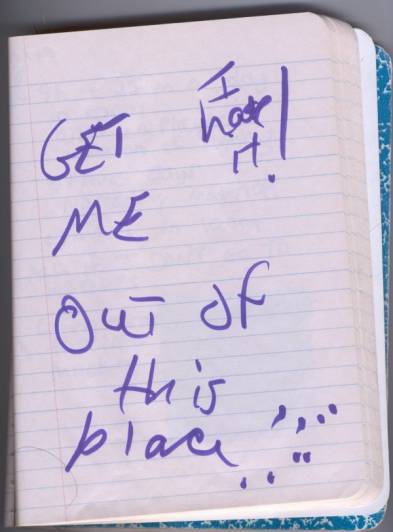
-From the journal of Petra, age 15,
1996.
Written while inside a state psychiatric
hospital.
HOME AND THE HOSPITAL:
A Study of Home
Elements Provided in Psychiatric Hospitals for Adolescent Girls
by Jane Schreck
Writing Workshop II:Ý Professor Julia Keefer
New York University
The purpose of this study was to see if psychiatric hospitals/hospital units on Long Island/New York provided elements of home for adolescent girls requiring intermittent inpatient hospitalization, in order to foster feelings of security, comfort and a sense of belonging.Ý A survey was developed to help to define which home elements are perceived as important to adolescents in both home and hospital settings. Surveys were given to ten middle class females, age 13-18, not diagnosed with any psychopathological disorders and thus not requiring psychiatric hospitalization. Psychiatric professionals, a staff member and a parent were interviewed for their opinion on this issue. Most agreed on itís relevance and cited quality, i.e. the degree of sensitivity/kindness of all hospital staffing along with family involvement/family therapy as the most important factors in providing nurturing environments.Ý They raised important financial and insurance issues. Four case study subjects were also surveyed, who currently are or previously were hospitalized between the ages 14-18, suffering from various psychopathologies, which necessitated intermittent inpatient care in Long Islandís psychiatric hospitals/hospital units. Their experiences and perceptions have provided much insight of the hospital environments, where they received or are receiving treatment.Ý The hospitals were rated based on home element criteria identified in this study. Most of the six hospitals studied were found to be blatantly lacking with some or all of the home elements, especially girls not feeling safe in some of the hospitals. Lack of financial resources, especially in state run facilities was a major factor. Other influences were type/size of facility, location and demographic population. Treating adolescents with adults poses a problem. One unit in a small hospital was found to be an ideal model. The case study subjects all agreed that the amount and quality of psychiatric therapy and activities plus family involvement/therapy provided in the hospitals was of vital importance in conjunction with a nurturing home environment for perceived overall benefit. Conclusion: managed health care is forcing shorter, more focused stays which may influence hospitals to provide intensive, effective programs. This could be an argument for creating a strong nurturing environment.Ý It could also be an argument against with relevance to budget constraints. Sensitivity training programs for all staff members, not just the professionals, could help create the nurturing family atmosphere where it is minimal or absent from hospitals. Further studies are needed to show the efficacy of a model nurturing environment by studying patient outcomes.
ìAt a time in my life when
I was frightened and in emotional pain I turned to psychiatry for help.Ý Sometimes things get to be too much for
people and they just need a break.Ý This
can happen to anyone, it can happen to you.Ý
If you canít take a break at home, the only other option in this society
‚ the place you go to, to get a little rest, where others will take up the
slack for you, care for you a bit -Ý is
the hospital, so they tell us. But they lie.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Shelagh Lynn Supeen, ìAs for the Sky: Fallingî
ìBut I donít want to go among mad people,î Alice remarked.
ìOh, you caínít help that,î said the Cat: ìweíre all mad here.Ý Iím mad. Youíre mad.î
ìHow do you know Iím mad?î said Alice.
ìYou must be,î said the Cat, ìor you wouldnít have come here.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Alice and the Cheshire Cat, ìAlice in Wonderlandî
ìIt was like being Dorothy in the Wizard of Oz.Ý All of a sudden you are completely uprooted and in a weird place.Ý Some of itís friendly and supportive. People want to help you find the way.Ý And some of it is as scary as the Witchís castle.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Kirsten, age 19
LETTER FROM HOME:Ý REFLECTIONS FROM YOUR RESEARCHER
Ý
ÝÝÝÝ Why should a researcher care about whether or not the psychiatric hospitals on Long Island
provide a home environment for teenage girls?Ý The strongest allure for a quest into the unknown
usually stems from a desire to know the truth, fueled by a personal experience, painful and real.
Such is the poignant draw for this researcher.Ý A teenage girl, very close to me, is currently
hospitalized in one of Long Islandís psychiatric hospitals.Ý The symptoms of her psychiatric
illness are no longer manageable with outpatient care and she has been confined in this facility
for the last five months, as of the date of this research report. She is severely homesick, misses
her family and wonders why is she being punished?Ý I wonder why she feels she is being
punished, why she can only be visited by one parent for a couple of hours once a week, and why
there doesnít seem to be a nurturing/homelike environment?Ý This question has led me on the
path of this research project.Ý Are most psychiatric hospitals on Long Island like this, or just this
one?Ý What constitutes a homelike/nurturing environment?Ý Is providing a nurturing environment
necessary or irrelevant to the ultimate healing of psychopathological disorders?Ý How do
professionals feel about providing a home in the hospital?Ý How do the teenagers hospitalized
feel about this question?Ý I wanted to address these questions through my research. And although
this study is inspired by the painful experience of a loved one, I nonetheless approach the task
Ýof looking for home in the hospital with objectivity and a commitment to seek the truth.
SETTING UP HOME: SECURITY, COMFORT AND A SENSE OF
BELONGING.
ÝÝÝÝ The concept ofÝ providing elements of home in the hospital for adolescent girls is not one
explored in great depth.Ý My rigorous search for case studies and information seemed fruitless at
times, yet is not a concept completely ignored.Ý Some psychiatric nurses recognize ill effects ofÝ
ìnon-nurturing environments.îÝ They prescribe supportive and home-like hospital environments
to lessen the effect of stress on the ìpsychological stabilityî of an adolescent.Ý An important
factor for our teenage girl who is hospitalized for her psychological instability. Nurturing
environments provide deep, healing, positive experiences for adolescents (Shoen Johnson, 1995).Ý
Conversely we could say if the environment is non-nurturing it would be a deeply negative
experience for our teenage girl who is already suffering. The environment sends powerful
messages that influence behavior, it can nurture coping skills and socialization, or promote
feelings of isolation and depersonalization (Olds, 1978, Pischeria, Bragg, & Alvaraz, 1982).Ý We
can see the value in considering the environment as an important factor in the healing process
because of its influence on behavior.
ÝÝÝÝ In this study, I define ìelements of homeî as anything that creates a nurturing
environment to promote feelings of security, comfort and a sense of belonging for the adolescent
female inpatient requiring intermittent hospital stays.Ý Intermittent is defined as a one to five
month stay for each individual, possibly repeated over a course of one to five years.
ÝÝÝÝ Security means feeling safe from harm, from self, staff or other patients.Ý It implies not
feeling anxious or fearful, the ability to ìrelaxî in the surroundings and not feel physically,
mentally or emotionally vulnerable.Ý Safety should be an issue in considering hospital
environments. Most psychiatric patients have confused thoughts and unchecked emotions, so
they could present harm to themselves or others (Berger & Vuckivic, 1994).Ý Teenage girls with
suicidal thoughts or violent behavior patterns would fit in this category of self harm/harm to
others.Ý I can imagine the difficulty for a teenager trying to heal from a psychiatric illness if she
feels physically threatened or feels further emotional insecurity from an indifferent, cold staff.
ÝÝÝÝ Since I consider homes as contributing to a model for hospitals, it is important to
acknowledge that some home environments of girls are not safe and secure, and are in
fact the contributing causes of psychopathological disorders.Ý Physical, sexual and emotional,
abuse and neglect prevail in many homes.Ý Home environments are routinely
assessed to uncover harmful/abusive vs. loving/supportive aspects (Schoen Johnson, 1995).Ý
I look for an overall ideal of a secure home rather than the dysfunctional one to
apply to the hospital setting.Ý I surveyed teenage girls for their concepts of home, who were from
relatively safe, secure homes, to serve as my control group.Ý The girls in my case studies, who
have psychopathological disorders, may or may not have come from safe, secure homes, but
were also surveyed to carefully consider their viewpoint.
Ý
ÝÝÝ Comfort is defined as that which soothes, makes life easy, and promotes feelings of
contentment. Comfort encompasses issues of privacy, personal space and familiar surroundings.
Hospital design should reflect comfort in the furniture, space and allowance for personalization
(Shoen Johnson, 1995).Ý Being comfortable involves not being uncomfortable, or feeling the
environment is cold, impersonal or physically unpleasant.Ý Studies show that cleanliness,
attractive dÈcor and quality of food are important considerations in hospital settings for patient
satisfaction and comfort (Squire, Stout & Reuben, 1993).Ý Comfort is an essential element in the
home to create a sense of peace. As stated by Witold
Rybczynski in his book, Home: A Short
History of an Idea, ìComfort was meant to be undramatic and calming.îÝ Most of us desire a
comfortable place to heal our mental and physical wounds in.Ý I know I certainly do.
ÝÝÝÝ Sense of belonging signifies relationships, family atmosphere and involvement in activities.Ý
The psychiatric hospital becomes the new temporary home.Ý Doctors, nurses and all staff
members become the surrogate family. Feelings of being loved, cared about and supported
constitute a healthy home and thus should be the goal of the hospital.Ý This is a therapeutic
environment: a team approach between empathetic, caring therapists, staff, family members and
the patients. As in the home, the hospital should provide the adolescent with structured daily
activities, rules, positive reinforcement for good behavior, the continuation of school work along
with individual, group and family therapies. (Shoen Johnson, 1995).Ý An adolescent girl in the
psychiatric hospital filled with a sense of belonging, is less likely to feel isolated, lonely or
homesick.Ý Besides avoiding these negative feelings, it is important to promote a family home-
like world to help build self esteem through support and approval. (Gelard & Gelard, 1999).Ý A
home/familial setting in the hospital could help the suffering teenager develop a positive self
image.Ý A sense of belonging means giving her personal space with individual touches to
promote self identity.Ý It promotes open relationships with the staff and a positive sense of group
identity.Ý (Lennard & Gralnick, 1986)
ÝÝÝÝ Elements of home in the hospital creates a therapeutic community as A. Gralnick, in
Humanizing the Psychiatric Hospital, beautifully describes:
ìAnything
that makes life easier and more comfortable is thought of as a mark of the
therapeutic communityÖAny place that gives the patient little cause for
complaint is the therapeutic community.Ý
Any hospital that is ëlike homeí is the therapeutic community.Ý An environment that is peaceful and permits
leisure time, pleasure and freedom from pressure is the therapeutic community.
Particularly, anything akin to the ëhumane approachí is considered therapeutic.î
(p.72)
ÝÝÝÝ
THEREíS NO PLACE LIKE HOME:Ý HOME TO THE TEENAGE GIRL
ÝÝÝÝ Home is our connectedness with people, a unique place, a past anchored with memories and a
future for dreams and hopes. (Altman & Werner, 1985)Ý A lovely sentiment, but as Clare Cooper
Marcus aptly put it in her book,Ý House as a Mirror of Self:Ý ìHome can mean different things to
different people.îÝ This is true for the teenage girl whose subjective choices are persuaded by
ìjunk values of a mass cultureî, as described at length in
Dr. Mary Pipherís book Reviving
Ophelia.Ý Open any magazine or look at television to see the media bombardment of carefully
marketed products targeted at teens.Ý Popular culture themes affect their tastes and preferences.Ý
Additionally the teenage girlís concept of home is influenced by family/parental choices and
controls. But whatever the influence, her concept of home as a nurturing, welcome place requires
exploration to provide a paradigm for the psychiatric hospital environment.Ý It is important to
solicit the opinion of the adolescent girl if we are to help her.Ý She should be involved in the
process of her treatment because she is at an age when she needs to be listened to with
understanding and acceptance (Shoen Johnson, 1995).Ý If we can find out what her needs are, we
can use this to influence her behavior, especially self destructive behaviors, like suicide attempts,
drug abuse, violent behavior, self-mutilation or eating disorders. The adolescent girl, like all
humans, have learned behavior which is affected by gratification through ìpay-offsî.Ý For
example if there is a positive pay-offÝ for doing homework or chores, she is likely to repeat the
behavior.Ý If wearing certain clothes or teasing a friend rewards her with compliments or
laughter, again she is likely to repeat the behavior. She learns from feedback she gets after the
behavior, thatís why adolescence is a time of experimentation and risk. (Boyd-Franklin & Bry,
2000).Ý If we find out the ìwhatís in it for meî values of the teenage girl, we can determine
criteria for providing a nurturing, therapeutic environment for her.
ÝÝÝÝ I developed a survey to help define which elements of home were of importance to teenage
girls.Ý I asked a Nurse Clinician at Mount Sinai Hospital and a member of a psychology honor
society to review the survey for their input and critique. (See attachment 1 for a sample survey.)Ý
Keeping in mind the ìwhatís in it for meî factor, I spent forty dollars on mini-perfume bottles as
a ìlook what you get for doing this surveyî reward.Ý Armed with my fragrant enticements,
dressed in floral decorated jeans and a t-shirt that said ìGirls Ruleî, my glitter decorated eyes
and I ventured out into the world where teenagers congregate.Ý I went to the mall.Ý I set out to
Ýfind ten middle class girls, age 13-18, who had never been hospitalized or diagnosed with any
psychopathological disorders.Ý I wanted them to serve as my control group against the four case
studies, whose homes may have had negative influences.Ý I approached a group of girls and one
said, ìCool eye shadow.îÝ I was accepted, however I only netted three surveys that day.Ý The
remainder I solicited through adults who had daughters willing to take the survey.Ý
Finally I had all ten surveys, plus four additional from the girls who were hospitalized.
ÝÝÝÝ The first part of the survey consisted of twenty open ended questions designed to get the
subjects to reflect deeply on home and personal values. This prepared them for a list of thirty
Ýìhomeî items that they were to put in order of importance.Ý They were asked to repeat this
process to consider home elements they would desire if they were staying in a hospital for a few
months.Ý This last part was the most crucial for this study and is what will be analyzed.Ý
ÝÝÝÝ It was expected that their answers would be very different but that collective themes would
emerge.ÝÝ I rated their answers as: essential, very important, moderately important and least
important.Ý When examining home elements in hospitals, I will consider the girls essential and
very important choices. They are listed on the following chart in order of priority:
|
Essential |
Very Important |
Moderately Important |
Least Important |
|
Spending
time with family Having
someone to confide in Spending
time with girlfriends Feeling
safe/secure Having
privacy Spending
time w/a boyfriend Wearing
cosmetics* |
Eating
home cooked meals Taking a
warm bath or shower Listening
to CD's Talking on
the telephone Feeling of
belonging/fitting in |
Watching
television/videos Having
leisure time Having the
freedom to go out Sleeping
in a comfortable bed Having
art/decorations Playing
with pets Having
personal "stuff" from rooms Having
exercise/sports equipment Playing on
the computer Wearing
favorite clothes Having a
cozy chair/couch |
Reading
favorite books Having
plants/flowers/garden Celebrating
birthdays/holidays Having
drawer/closet space Eating
junk food Playing
video games Studying
at oneís own desk Wearing
cosmetics* |
Fig.
1ÝÝÝÝÝ *This is listed twice because all four
hospitalized girls ranked this in their top five while the entire control
Ýgroup listed it as their last priority! This
was the only element that had such a marked difference, so I felt it worthwhile
to note it here.
ÝÝÝÝ Spending time with family was the number one value. It ranked in the top three for all girls,
except for one of the girls hospitalized for anorexia. A possible explanation for this
would be that she felt she did not have a good relationship with her mother.Ý She perceived this
as part of the cause of her illness and did not value spending time with her family.Ý Families are
at the core of the home and the girls value this above all. This is a strong argument for family
involvement and family therapy in the treatment plan.
ÝÝ
Ý Having someone to confide in ranked as the second most important element and was a top three
choice for the four hospital patients.Ý Girls want to unburden their souls to a person they trust.
This could explain the high ranking for spending time with girlfriends and spending time with a
boyfriend, for the few that had steady boyfriends.Ý Therapists, nurses and staff have to create that
umbilical cord of trust so crucial in helping their teenage patients open up.
ÝÝÝÝ Feeling safe/secure was essential to all four case study girls and most of the control group, as
was having privacy.Ý Most complained about not having privacy in their own homes.Ý Privacy is
difficult to have in a public setting, especially a hospital.Ý In order to provide safety/security for
the teenagers in the hospital, individual privacy has to be compromised.Ý Still, where it is
feasible, privacy issues for bathrooms, showers, personal space could be considered to cater to
this need.Ý Privacy associated with the stigma of being hospitalizedÝ is taken very seriously by
hospitals.Ý Most try to protect outsiders from gaining any information about a patient.Ý
ÝÝÝÝ Wearing cosmetics appears in both essential and least important categories.Ý This
was a curious division among the hospital patients and control group.Ý I attempt a possible reason
for this: sometimes teens tend to want what they canít have.Ý Some of the first things taken
away from teenagers upon admission into a psychiatric hospital are their cosmetics.Ý It is part of
standard hospital procedure to confiscate anything that can be broken into sharp objects to use in
suicide attempts, self-mutilation or as a weapon.Ý The case study group may have changed their
priority on this, if they were told their cosmetics would be confiscated for a few months.Ý
Allowing for cosmetic packaging made of unbreakable soft plastic could be a solution if such
products exist.Ý If not, this perhaps is yet another untapped market for cosmetic companies!Ý
ÝÝÝÝ Eating home cooked meals was very important to all of the girls except our anorexic patient
for obvious reasons.Ý Based on the comments the hospitalized girls made, providing quality food
is/was overlooked in most of the hospitals, not surprising for any of us who have had the
pleasure of being served ìinstitutional food.îÝ One girl said the food in Dragmont Hospital was
literally thrown together and barely edible.Ý An interesting point is that all girls rated junk food as
least important, a fact that would please most parents.Ý Food is strongly associated with home.Ý In
the survey, all the girls describe different home cooking smells as what they like about home.Ý
I believe providing quality, well prepared food is part of the therapy.
ÝÝÝÝ A true mark of the passage from childhood to adolescence is the desire to take baths and
showers without parents asking!Ý The proof is in the girls rating this as very important.Ý Also
important was listening to CDís and talking on the telephone, which are not surprising
choices, and are considered perks as part of step up programs in most hospitals. Lastly, the girls
want to feel like they belong and fit in, they donít want to feel alienated.Ý I suggest creating the
home in the hospital to help foster those feelings.
ÝÝÝ This survey provides insights into what girls value and need for healing.Ý Applied to a hospital
setting, the staff must be nurturing and create heartfelt bonds with the girls in addition to
allowing frequent visits from family and close friends.Ý They need to be aware of privacy and
safety issues and become the confidante for these girls and help them feel like they belong.
Good food, a pleasant place to take a hot shower, allowing music and telephone privileges
are adolescent priorities.Ý Stewart D. Govig (1994), describes a ìpleasant inpatient environmentî
as having ìa corps of aides, nurses and others ‚ who stay with patients around the clock to
provide food, comfort and security.î (p. 29)Ý
THE HOME TEAM-DOCTORS, NURSES, STAFF AND PARENTS
ÝÝÝÝ Anxious to get the opinion of professionals regarding this study, I obtained interviews with
Dr. Selma Goddard,Ý Dr. Harry Tonla,Ý Janet Cooper R.N. and Kathleen Switzer, parent to a
hospitalized teenager.Ý Two of the interviews transpired briefly in person, two by telephone.Ý I
changed all names as requested.Ý I am grateful to all for taking time from their busy
schedules to work with a budding researcher.Ý I asked if they thought this was a relevant
issue and what their insights were.
Dr. Selma Goddard, Behavioral Therapist
ÝÝÝÝ ìThe idea of creating a nurturing
environment is absolutely relevant.Ý I
have three words that describe what can make a home environment: staff, staff,
staff.Ý Having a cold, impersonal staff
when kids are already scared to death, exacerbates the situation.Ý The staff should create as much warmth as
possible to aide well being.Ý They have
to give individualistic kindness and treatment.Ý But, I must say, this is very difficult to do when they are short
staffed and they have to follow hospital rules and regulations.ÝÝ Or a hospital may have a great program in
theory but the nurses are overwhelmed and overburdened.Ý There are aides that help out, but if they
are not English speaking, they are not going be able to communicate.Ý And communication is key!Ý Every patient needs an advocate to protect
their patient bill of rights, even high level places.Ý
ÝÝÝÝ There are many, many philosophies in
psychiatry.Ý I am an eclectic therapist,
I like to draw from many sources to provide a plan A, a plan B and so forth for
my clients.Ý I look for an individual by
individual approach.Ý I am aligned to
the fact that patients are people.Ý
Professionals need to really, truly care about the person and have
kindness.Ý Creating the home environment
depends on whether or not the staff and therapist are there for the
teenagers.Ý Itís a vital point.Ý They categorically must be there for the
patient.Ý Home is security, caring,
loving.Ý Staff has to be aware and want
to help.Ý
ÝÝÝÝ The teens rooms are their
private spots, they should be allowed some personal items.Ý Their own blanket, wearing their own clothes
instead of hospital gowns.Ý They should
wake up and see drawings, pictures theyíve made. ÝStereo and CDís are so important to kids.Ý Take all the sterile crap out of the
hospital, the teen should not be a statistic.
ÝÝÝÝ Some hospitals give the illusion they are there for the patient, but itís a lie!î
Dr. Harry Tonla, Psychiatrist
ÝÝÝÝ ìOf course, this is a
relevant issue.Ý Most hospitals are not
known for their comfortable atmosphere.Ý
I have worked with many adolescents in psychotherapy.Ý They could definitely benefit from this kind
of home-like environment, but what is feasible? You have to remember hospitals
are businesses.Ý Are they in the
business of healing people?Ý Yes, but
secondarily.Ý They are in the business
of making money first.Ý And this is the
biggest problem all medical doctors have who work in hospitals. You are
fighting for money for your unit, your programs.Ý You are dealing with an administration as complex as the diseases
we treat.Ý But Iím am not saying it
shouldnít be tried, in fact some hospitals do have very good programs for
teenagers, but there is always room for improvement. I bring the issue of
finance to the table because this is real life.
ÝÝÝÝ The other enemy to good treatment is the
insurance companies.Ý As a
psychotherapist, this is a heinous problem.Ý
Therapy takes time and it is not fair to push patients out the door
because their insurance has run out.Ý Do
you realize the decline in the number of days for inpatient
hospitalization?Ý About ten years ago
you might stay for ninety days, today because of the decisions made by the
managed care people, you may only stay for ten days.Ý Soon you will have a drive through window!Ý I am not saying the goal should be to keep a
child in the hospital for three months, in fact that is not the philosophy
today. But for the seriously ill patient, to shorten their stay because of
insurance seems ludicrous to me.Ý
Discharging them prematurely could have disastrous results.î
Janet Cooper, R.N. ‚ Staff nurse at Mother Hospital
ÝÝÝÝ ìWe definitely strive for a caring
environment. We are very small, we have only ten beds.Ý This is our ninth year here and we have all
the original people who started this program. We created the program and have
evolved and improved it over the years.Ý
We have a nurturing environment and we really care about the kids and we
treat them with respect.Ý The stability
of staff is key.Ý We have four full time
masters degree level and one part time bachelors degree level. So our staff is
professional.Ý We have very specific
programs, we are very much into family therapy.Ý We have sessions every day, one on oneís, group, art class.Ý The kids have goal sheets and they are given
specific plans. We give out a lot of printed materials to kids and their
families to educate them.
ÝÝÝÝ Managed care has definitely affected the
length of stay for patients, sometimes they only stay for nine days at a time,
depending on the problem. It is very challenging.Ý We have to intensify efforts to help our patients.î
Kathleen Switzer- parent of an inpatient teenager.
ÝÝÝÝ ìMaking a hospital like home
is a very important goal. My daughter has been through what we parents jokingly
call the Long Island Leap Frog.Ý Our
kids have gone from hospital to hospital, because of doctors preference,
insurance or money issues or not enough room. I could write a book about all
the experiences Iíve been through with the hospital system.Ý It is so hard to deal with having a sick
child. You end up feeling guilty and blaming yourself for her illness.Ý But there were some terrible factors that
led to my daughters hospitalization. I can honestly say my husband and I have
been there every step of the way for my daughter though this whole nightmare.
ÝÝÝ To make a home place, the people are
crucial.Ý Some of the staff are so
professional and welcoming to families.Ý
They have excellent programs and give you a lot of information so you
donít feel in the dark.Ý ItÝ can be so confusing with the diagnosis and
the drugs they prescribe. You have to be in constant communication with
them.Ý Some are very accessible, some
are not.Ý Some hospitals are terrible.Ý The staff is evasive, or they donít have
much time for you or your child.Ý Some
of them are downright abusive.Ý My
daughter was so traumatized by one place that I wanted to take her home.Ý I will never forget what the Doctor said to
me, it chills me every time I think of it. He said, ìYour daughter will be dead
in a year.îÝ Probably if she had stayed
in that hospital she would be.Ý
ÝÝÝÝ The most important thing I can say is you
have to speak out and fight for your kid and make sure they are getting everything
they are entitled to and not falling through the cracks.Ý Are they getting their therapy?Ý Are they getting help?Ý I found the hospitals that had a variety of
therapies really helped my daughter.Ý
And family therapy helped all of us, because a childís illness affects
everyone in the family.
ÝÝÝ The paperwork is absolutely endless, the
insurance forms, the hospital forms, it never ends.Ý And there are constant battles with the insurance companies.Ý They donít want to cover this or that. The
best thing is to put your kid in a private hospital.Ý But they are so expensive.Ý
For example, therapy that cost $1300 in a state hospital cost $7000 in
the private hospital!Ý That is
outrageous, but what do you do, sacrifice your kid?Ý The insurance companies donít cover it all for private hospitals.
This whole managed care thing forces the kid to be discharged before sheís
ready.Ý We are already going through
hell with having a sick child, we donít need this bull shit from an insurance
company.î
ÝÝÝÝÝ
ÝÝÝÝ Dr. Goddard, Ms. Cooper and Ms. Switzer recognize staff quality as an integral part of the
nurturing environment.Ý In dealing with adolescent psychiatric programs, qualities of caring,
personal contact, commitment and how well the staff relates to adolescents seems to be
associated with program success. (Brooks-Gunn & Foster,Ý 2000)Ý Staff has to be fully involved,
not neutral, but biased, in a truly loving, and safe relationship.Ý (Kennedy & McCarthy, 1998)Ý I
agree with a philosophy of professional credentials plus a vocational calling to work with
adolescents.
Ý
ÝÝ ìOur
familiesÖwere utterly absent from our hospital lives.îÝ This quote from Susanna Kaysen
in her book ìGirl, Interrupted,î could
have been written by my case study, Beth, whose
hospitalís philosophy is to distance
family from the treatment process.Ý Ms.
Switzer talks of the
importance of communication between staff
and family.Ý An adolescentís
psychopathology
greatly affects the family.Ý Parents are already bewildered and canít
make sense of extremely
disturbing behaviors in their
daughter.Ý They donít know how to
respond. (Karp &
Tanarugsachock, 2000)Ý Ms. Cooper prescribes family therapy . The
treatment team should want
to foster good relationships with the
patients family.Ý Obviously this makes
the work of healing
the patient have a better chance if
everyone is working toward the same goal.Ý
(Korpell, 1984)Ý
The American Nurses Association advocates
that families should be included in the treatment
process. (Mohr, 2000)ÝÝ
ÝÝÝ Dr. Tonla raises important issues with regard to finance.Ý Is my search for home in the hospital
all for naught if there arenít sufficient resources?Ý Dr.Goddard talks of the problems of
insufficient staffing and nurses who are ìoverwhelmed and overburdened.îÝ Budget constraints
to limit staff or cut programs will definitely affect quality.Ý Ms. Cooper and her co-workers are
able to provide a nurturing environment in a small unit of a private hospital where more
resources are available.Ý Ms. Switzer prefers putting her child in a private hospital but points out
the exorbitant costs; the downside of getting quality healthcare.Ý She doesnít want to
ìtraumatizeî her daughter by putting her in ìterribleî hospitals, but how can she afford it?ÝÝÝÝÝ
ÝÝÝÝ Which brings me to the most frustrating factor for doctor, nurse and parent: managed
health care.Ý Professional agree that the interference of healthcare systems to interrupt psychiatric
care will negatively affect the healing process and outcome.Ý (Masters, 1997)Ý Patients discharge
planning often coincides with the date the insurance benefits run out, regardless of patient,
doctor or family wishes.Ý (Sharkey, 1994)ÝÝ Dr. Tonla humorously points out the trend of
shortening the inpatient stay with his ìdrive through windowî prediction.Ý I found entire web
sites devoted to managed care humor, like the following cartoon:
 ÝÝÝ
ÝÝÝ
ÝÝÝÝÝÝÝÝ North County Psychiatric Associates.
ÝÝÝÝ Managed care is an argument for home in the hospital, by forcing an intensive, therapeutic,
effective hospital stay.Ý Or it is an argument against by prescribing a no frills, stabilize and
release philosophy.Ý Pro or con, it is the source of controversy and frustration for all.
TEENAGE WASTELAND: THE TEENAGE GIRL WITH PSYCHOPATHOLOGIES
ÝÝÝÝ Adolescence is the rickety bridge between childhood and adulthood.Ý It is the time of rapid,
profound change.Ý Puberty, in Websterís dictionary, deals with biological readiness for
sexual reproduction.Ý This simple definition leaves out the emotional, social and physical angst
that adolescentís experience. As though at a carnival, they ride the hormonal roller coaster, get
horrified by distorted fun house self images and get trapped on giant pendulum ships, moving
from childhood to adulthood and back again.Ý It is a time of excitement and ìfrightment.î
Teenage girls are at particular risk during this time. They are overwhelmed by an oppressive,
media-worship culture; pressured to be sexy, beautiful and sophisticated while feeling the
awkwardness of their evolving bodies. They go inward, become more secretive, internalize hurts
and confusions.Ý (Pipher, 1994).Ý It is no wonder that the rate of psychopathologies increase
during adolescence. (Steiner & Yalom, eds., 1996)
ÝÝÝÝ I felt it important to examine the predominant disorders affecting my four case study
teenagers.Ý It would be impossible to explore all adolescent psychopathologies in this research
paper, since the main focus is on looking at home elements in the hospital.Ý I wanted to
consider what special needs the girls might have because of their illnesses.Ý All the girls were
found to have multiple disorders, but these four dominated their diagnosis: major depression,
drug addiction, anorexia, and obsessive-compulsive disorder.Ý The reflective nature of this next
section, in no way attempts the depth of complexity that these disorders deserve.Ý This is meant
merely to offer another perspective on the issues of security, comfort and sense of belonging.
ÝÝÝÝÝ Categorizing psychopathologies is not an exact science.Ý I found conflicting information, but
selected an excellent comprehensive text by Steiner & Yalom eds., which bases the categories on
the Diagnostic and Statistical Manual of Mental Disorders (DSM-IV).Ý I created the table below
to highlight the four disorders and show what category they fall under.Ý This is an abbreviated list
and does not include every single psychopathology.
Ý
|
AFFECTIVE DISORDERS |
ANXIETY DISORDERS |
DISRUPTIVE BEHAVIORAL DISORDERS |
EATING DISORDERS |
SUBSTANCE ABUSE |
OTHERS |
|
Major Depression Bipolar Dysthymia |
Panic Phobias General Anxiety OCD |
ADHD Conduct Disorder Oppositional/Defiant |
Anorexia Nervosa Bulimia Nervosa |
Alcoholism Drug Abuse |
Schizophrenia Psychotic Disorders Psychiatric Trauma |
Fig.
2Ý
Major Depression:
ÝÝÝÝ Major depression is the most extreme of all the affective disorders and manifests as a feeling
of profound sadness.Ý Teenagers with major depression may exhibit sleeping problems, loss or
increase of appetite, weight fluctuations, trouble concentrating or a focus on suicidal ideology.Ý
They can no longer do all the things that they used to do, like schoolwork, part time jobs, sports
or social activities.Ý They can lose interest in appearance and personal hygiene or engage in
promiscuous sexual activity.Ý An overall feeling of not caring pervades.Ý At itís worst it can lead
to suicide, alcohol and drug abuse, total failure at school or increase in risky behavior.Ý
Teenagers at high risk for major depression include those with a family history of depression or
substance abuse, those who suffered trauma or abuse and those whose families are going through
divorce, marital conflicts or problems with children. Girls have a higher rate of depression at
puberty than boys.Ý Poor body image may be one reason girls feel more unhappy, anxious and
unattractive than boys. (Steiner & Yalom, eds., 1996)
ÝÝÝÝ Hospital staffs have specific strategies for dealing with suicide risk patients.Ý They may
assign a nurse to a patient for a one on one watch to get the teenager through the dangerous
period.Ý (Shoen Johnson, 1995)Ý As mentioned earlier, anything that can be used for a potential
suicide is confiscated.Ý This includes use for self harm as well as suicide. Girls are increasingly
engaging in self mutilation as an outer physical expression of their inner anguish (depression).Ý
(Piper, 1994)Ý Two of my case study girls, Petra and Kirsten, showed me their scars as a result
of this destructive practice.Ý A chilling reminder ofÝ how deeply the girls were wounded on the
inside. Another factor with suicide patients is the idea that suicides can occur in clusters.Ý
(Gould, Wallenstein & Kleinman, 1990)Ý
ÝÝÝÝ My home element of safety is at stake here. A girl with major depression and suicidal
tendencies needs a vigilant, sensitive staff to recognize symptoms for intervention and to keep
the environment safe.Ý Awareness of the influence teens have over each other is key. I think this
implies getting to know the girls and who their inpatient friends are.Ý Like a good parent, the staff
needs to be on constant watch for signs of trouble. Teenagers can be very creative in their drive
to obtain implements of harm.Ý Case study Danielle assisted Petra with a smuggled shoelace
noose.Ý I want to suggest that all staff members be vigilant in this matter, not just doctors, nurses
and social workers, but the cleaning woman, the cook, the aides etc.Ý This may be a philosophy
in certain hospitals but I was unable to obtain that information about the six hospitals in this
study.Ý
ÝÝÝÝÝÝÝÝÝÝÝ

Ophelia
by J.E. Millais depicts a scene from Shakespeareís Hamlet.
Works
of Art have sometimes romanticized suicide. (Chiles, 1986)
Drug Abuse:
ÝÝÝÝ The staggering amount of information on teenage alcohol and drug abuse available is
astounding to me and implies the serious prevalence of this problem.Ý Dr. Les Parrott III, author
of Helping the Struggling Adolescent, describes the following warning signs:
ìÖ social withdrawal, deterioration in school performance, resistance to authority, behavior problems, high-risk behavior such as stealing, extreme mood swings (which include signs of depression), sexual promiscuity, physical complaints, changes in relationships, changes in eating habits, and the more observable signs such as alcohol on the breath, slurred speech, staggering, appearing ìspaced out,îÝ dilated pupils, the presence of drug paraphernalia ( pipes, pill boxes, straws, spoons), and clothing depicting drug themes.îÝ (p. 125)
ÝÝÝÝ My research turned up volumes of theories on the reasons why a teenager becomes
addicted.Ý There are many physiological, genetic, social, peer pressure, media, familial and
psychological factors which donít need to be defined in this study.Ý Rather my focus is on the
issues of inpatient treatments and how this will relate to our home elements.Ý One big problem
identified, is the grouping of adolescents with adults for treatment, rather than recognizing their
different needs.Ý If teenagers find themselves in group therapy, surrounded by adults, they may
feel very uncomfortable and never benefit from it. The traditional model looks at physiological
and genetic factors which excludes the psychological aspect prevalent in teen drug abusers.Ý If
teens are lucky enough to be placed in an available adolescent unit, there is still the mixing of
drug and alcohol abusers who need different considerations. Different levels of abuse require
locked or unlocked units.Ý A patient may not be placed in the hospital that can best suit her needs
(Steiner & Yalom, eds., 1996)Ý I agree with this and identify it as the home element, sense of
belonging/fitting in, as in fitting in with the right hospital setting.ÝÝ Case study Danielle,
had a cocaine addiction and mild manic/depression. Fortunately she was treated in an adolescent
only unit that was psychiatrically and medically oriented to deal with both her issues.ÝÝÝÝ
The
Scream by Edvard Munch.Ý
For
drug abusing teenagers, anxiety can reach
levels
of intolerable intensity. (Chiles, 1986)
Anorexia Nervosa:
ÝÝÝÝ ìYou canít be too rich or too thin.îÝ The frightening prevalence of the later part of this
mantra, has provoked a dangerous modern disease of young women that proves the opposite.Ý
You most certainly can be too thin. Everywhere one looks, thinness is idealized. Every day there
is a new diet or a new exercise machine to be bought from an infomercial.Ý
ÝÝÝÝÝ Anorexia Nervosa is one of the most difficult psychopathologies to treat and has the highest
fatality rate.Ý (Piper, 1994.)Ý Anorexics are hungry all the time but obsess themselves with
silencing their appetites. (Steiner &Yalom, eds., 1996). They eat low fat foods and no calorie drinks,
they eat slowly, hide food so people think they are eating, use laxatives and diet pills, engage in
excessive calorie burning activities, throw up food and develop little rituals.Ý It is ironic that a
disease that begins as a idea of beauty turns into unhealthy ugliness.Ý Concentration camp
thinness, dark hair growing all over the body for warmth and blackened teeth from incessant
vomiting; it is this image that the anorexic has twisted into beauty, and it is hard to convince
her otherwise. At seventy nine pounds, case study Kirsten still didnít feel thin enough!Ý It is no
wonder therapists are frustratedÝ when attempting to work with anorexia.Ý The therapist must be
committed to a long, arduous process, working with a medical doctor and nutritionist.Ý
(Steiner & Yalom, eds., 1996)
Ý
ÝÝÝÝ Several sources for my research mentions family therapy as being the most important in the
treatment of anorexia.Ý The reason for this, is that it is believed that the relationships in the
family helped create the disease. Parents who are obsessed with the child/adolescentís physical
and mental functioning to the point that their actions hinder individuation and separation from
the parent/child relationship.Ý (Shoen Johnson, 1995)Ý The child/adolescent in this situation
becomes the center of family conflicts, often playing one parent against the other. The parents
may then turn the blame on the child. Thus the anorexic gets used to putting her parents conflict
on herself. (Minuchin, Rosman, & Baker, 1978)
Ý
ÝÝÝÝÝ Families are highlighted again as an important home element.Ý Besides creating the surrogate
family, hospitals need to consider the real family and actively engage them in the process of
healing with family therapy, especially for the anorexic.

Girl
at the Mirror, by Norman RockwellÝ
A
young woman strives to be beautiful, butÝ
in
the
end anorexia takes on a life of its own.
Ý(Piper, 1994)
Obsessive-compulsive Disorder:
ÝÝÝÝ A typical day for a person with OCD, is a continuous repetition of rituals that destroy
emotion, time and the joy of life.Ý Its roots are in fear and anxiety.Ý Uncontrolled thoughts turned
into uncontrolled actions.Ý This last of the psychopathologies to be examined is perhaps the most
relatable.Ý We all have all had haunting thoughts that trouble the mind over and over again.Ý And
we have all had irrational impulses that we are compelled to act out.Ý The difference for us is that
we are able to stop and continue on with the flow of life.
ÝÝ
ÝÝÝÝ It has been suggested by Dr. Les Parrott III,Ý the reasons why teenagers becomes OCD may
be rooted in their attempt to reduce fear, control self-doubt, alleviate guilt through perfectionism
and live up to unrealistic expectations of parents.Ý The National Anxiety foundation suggests a
biological link with serotonin and therefore is treatable with several different medications.
Unfortunately finding the right combination may involve painful trial and error, as was the plight
of case study Beth, who underwent some terrible side effects until the right combination was
found.ÝÝ Dr. Parrott prescribes a three way therapeutic approach including behavioral techniques,
cognitive techniques and exposure to stimuli.Ý So treatment might involve relaxation methods to
deal with anxiety, using daily records to note obsessive thoughts to begin the process of altering
thought patterns and slowing desensitizing the adolescentís fear.ÝÝ I knew a young
man who had OCD.Ý He would constantly stop his car because he feared he ran over someone.
His therapist actually went out driving with him to help him by exposing him directly to the fear.
ÝÝÝÝ One could imagine the stigma associated with the actions of the OCD teenager.Ý Ridicule and
ostracizing would further induce anxieties.Ý Beth told of painful incidents of cruel comments that
haunted her to the point of exacerbating her OCD.ÝÝ She felt others avoided her and she had
trouble making friends.
ÝÝÝÝ I consider two vital elements for the OCD patient: creating a sense of belonging and
providing frequent, appropriate activities.Ý The staff can encourage a welcoming environment for
the OCD girl, where she does not feel perceived as weird but rather healing from an illness.Ý
Exposing her to others with similar problems and quality group therapy prevents feelings of
isolation. Also, the question of quality and amount of activities becomes important too.Ý
Hospitals can provide exercise or yoga classes, along with journal writing and other cognitive
therapies.Ý Boredom and lack of activities dominated some ofÝ the girls experiences in certain
hospitals, with lack of physical and mental activities.Ý Hours of TV watching is certainly not
therapeutic.
ÝThe Anguish of OCD, artist unknown.
Ý (National Anxiety Foundation,
2001)
ÝÝÝÝ My research of these four psychopathologies persuades me to ask some additional questions
about the hospitals in this study.Ý
Do they have:
- Close relationships with patients and vigilant watch over them?
- Family therapy?
- Segregation of adolescents from adults?
- Special units or considerations for different psychopathologies?
- Supportive environment to reduce anxieties?
- Varied multidisciplinary activities?
ÝADOLESCENTS IN WONDERLAND ‚ FOUR CASE
STUDIESÝÝÝÝ
ÝÝÝÝ The four case studies presented are white, middle class females, ranging in ages (at the
time of hospitalization) from 14-18.Ý All were hospitalized for multiple psychopathologies,
multiple times.Ý Collectively they stayed in six different hospitals on Long Island.Ý I struggledÝ
with the choice ofÝ presenting long excepts vs. pertinent quotes, but I believe the longer passages
strongly demonstrate, existence or lack of, home elements in the hospital. The girls stories are
fascinating and moving. Similar experiences overlapping the hospitals made it unnecessary to
transcribe all of the interview material, avoiding redundancy.Ý I included the girls memory of a
hospital if more detailed or significant.Ý I changed the names of teenagers and hospitals for
privacy and legality issues.Ý I left out some details contributing to their illness and leading to
hospitalization, which were very serious, traumatic issues.Ý This was at the girls request.ÝÝ I feel
very grateful to these four girls for their candor, bravery, poignancy and wit in revelations of an
anguishing adolescence.
ÝÝÝÝ PETRA
Petra is twenty years old and has been in and out of hospitals from age 14-18.Ý Of all the case
studies, her experience was the most extensive, with intermittent stays in five different
psychiatric hospitals/hospital units:
- Mother Hospital in Port Hamilton ‚ Special Adolescent Unit
- Dangerfield State Psychiatric Center
- Birmington Hospital ‚ Psychiatric Unit
- Dragmont Childrenís State Psychiatric Center
- Rocky Stream University Hospital ‚ Psychiatric Unit
ÝPetra had numerous suicide attempts and suffered from major depression, some bulimic
episodes and sleep disorders.Ý
Petra at
Mother Hospital:
ÝÝÝ ìI was fourteen years
old,Ý I was very depressed and plotting
my suicide, planning it in my journal.Ý
My therapist, Patrice wanted me to have a psychiatric evaluation. She
told me to pack a suitcase.Ý I felt some
relief, but not total relief because I knew my parents didnít know how bad I
really was.Ý Part of me wanted to say,
ìOh, Iím fine, forget the whole thing,î because I felt guilty about my parents,
but I knew that I really wasnít fine.Ý
ÝÝÝÝ I had to get evaluated by the director of
the adolescent unit at Mother Hospital.Ý
I packed my Muttsy, my stuffed animal I had since I was seven, this old
raggy little dog that I loved.Ý But they
go through your suitcase when you get admitted.Ý I couldnít have shoelaces because I was a suicide risk. If youíre
a suicide risk you canít have shoelaces, or a belt. If you need to hold your pants
up you get basically this thin piece of string, like yarn, if even that.Ý No one was allowed anything sharp, for
everyoneís safety and the staffís safety.Ý
And they wouldnít let me keep my stuffed animal because, people could
smuggle stuff inside of things. They go through everything looking for
ìcontrabandî as they call it.Ý No drugs,
no alcohol, no pills, no razor blades, knives, tweezers, no glass, no
mirrors.Ý That was pretty hard as a
teenager, not to have mirrors.Ý They had
mirrors in the bathrooms, but they were like this plexi-glass stuff, so you
couldnít break off pieces and try to kill yourself.Ý Everything there had grounded electricity, so thereís no way you
could electrocute yourself.Ý You
couldnít have your door closed.Ý
ÝÝÝÝ Sometimes I would have a private room,
but there were only two private rooms on the unit so mostly you had to
share.Ý You were allowed to wear you own
clothes, but they had rules for that too. No shirts that exposed midriffs, or
anything like that.Ý One time when they
put me on 4S, which is a suicide watch. They took everything out of my room,
everything, even the bed sheets and comforter.Ý
I had to lie on the bed with just a hospital gown on.Ý I was only allowed a blanket at night.Ý I was on a one to one watch, so someone was
with me 24 hours.Ý Some of them would
even come into the bathroom with you, others would be nice and just stand
outside the door.Ý The rule is they
needed to legally be in arms length of you at all times. They had to be able to
grab you just in case.
ÝÝÝÝ Mother Hospital was really the best. Each
room had a private bathroom.Ý And it
seems every single hospital Iíve been in always had the psychiatric unit in
something ìnorthî. 2 North, 5 North, 10 North.Ý
The room was pretty nice, it was plain, but the furniture was homey
looking.Ý When you were not on suicide
watch, they let you have pictures, but not in frames, and you could tape up art
or whatever you wanted.Ý As long as it
wasnít things like ìMarijuana is greatî or a suicide note or ìmy life sucksî or
something like that.Ý There also was a
rec room, but they called it the day area, with a foosball table, a T.V., and
separate couches so you could sit privately.Ý
And they had Nintendo, but you had to have certain level privileges to
play it.Ý They had a CD player/radio,
but there was a lot of rules with it, you could only have it for ten minutes at
a time.Ý You werenít allowed to have
your own walkman, this is something I really wished they allowed because music
is so important to teenagers.Ý Kids got
into fights all the time about the radio.Ý
And they didnít want us listening to certain music.Ý I liked the group Hole, but the cover of the
CD showed a girl with her wrists slit, so they banned stuff like that.Ý No suicidal ideology, or curses or drug stuff.Ý They made a rule later on that if you
brought in CDís you had to have a booklet of the lyrics so they could read them
first.Ý
ÝÝÝÝ The day area was nice, thatís where you
could visit with your family and they were allowed to come every day in the afternoon
and evening.Ý Your family could bring
food, but you had to be at a certain level to have a snack stored for you in
the kitchen.Ý When you first arrive at
the hospital, you are at level 1 which means you donít really have privileges
to go on off the unit activities.Ý If
youíre on level 1 you go to bed at 9:00 in Mother hospital, level 2 you stay up
till 10:00 weekdays and 11:00 on a Friday night.Ý Level 2 with a note from your Doctor, you could go to the other
units for arts and crafts, play games. They had a pool table.Ý At this point the staff and doctors had
observed you and you werenít considered dangerous to yourself or the other
kids.
ÝÝÝÝ The staff really was great at Mother
hospital.Ý One time we were all upset because
one of the girls who had gone home, ended up killing herself.Ý She was one of my friends.Ý I really took it hard.Ý The nurses were really nice and let those of
us on level 2 and 3, go off the ward entirely to go to a candy vending
machine.Ý I donít know what possessed
me, but it was the dead of winter, at night and I just bolted from the
hospital, out of the emergency room doors, I just ran, it was an impulse.Ý I ended up somehow in the backyard of some
Happytime Nursing home with no jacket and shoes with no shoelaces.Ý I realized, ìItís cold, what am I doing?î,
so I went back on my own.Ý They had
police and guards out looking for me.Ý I
remember walking back through the emergency room doors and some police officer
asked me, ìAre you by any chance from 2 North?îÝ I said, ìYeahî and he said,î A lot of people are really worried
about you.îÝ But he was really nice
about it and took me back to the unit and said to the two nice staff people,
ìNow go easy on her, she came back on her own.îÝ But those two nurses were really mad at me and wouldnít talk to
me for a week.Ý They really acted like
family, they were hurt that they trusted me and I betrayed the trust.
ÝÝÝÝÝ We had community meetings every morning
after breakfast where you could bring up all the petty stuff.Ý Then we had school for a few hours, the
tutors would come in they were pretty nice.Ý
You would get homework from your school district and the tutors would
help you.Ý If you didnít have anything
they would always give you something, they had good teachers there. We had
cooking class, we played games, or you would make something, art or
poetry.Ý We had relaxation class every
night, they would play music, we would lay down, and that was supposed to get
you calmed down before bed.Ý We had some
free time during the day, a couple of hours.
ÝÝÝÝÝ You were on a point system, you would
get points for doing good things, like making your bed, going to breakfast,
taking your shower.Ý Rather than the
opposite where would get points taken away if you didnít do them, which was the
case in other hospitals.Ý This was a
more positive system.Ý You would get
points taken away, like if you cursed. You also started out with points. If you
got higher points you would get more privileges.Ý If you made a certain level, the hospital unit got points, and
once a week you would go on a trip with a recreational therapist and one of the
staff, to the movies, bowling, or go to sports plus. There was a rule too that
you couldnít have any physical contact.Ý
It was coed, so no hugging or kissing.Ý
You werenít supposed to hug the staff either.Ý But I got plenty of hugs from the staff.Ý That was one rule they didnít enforce, they
were very loving.Ý
ÝÝÝÝ We got our meds in the morning and at
night.Ý Some people used to cheek their
pills, so they could store them up. They would make you open your mouth and
check to make sure you swallowed.Ý They
knew almost every trick in the book.Ý
Once before going back to Mother, I knew I wanted to have my
tweezers.Ý I took a stick deodorant,
which they let you have, and I rolled out the deodorant stick. I took my
tweezers and I wrapped it in paper towel and stuck it in the bottom of the
empty container and then put the stick back on top and rolled it down. So I was
able to keep my tweezers. I didnít want to hurt myself, I wanted to pluck my
eyebrows.Ý You werenít allowed to shave,
you had to be hairy the whole time.
ÝÝÝÝ I made friends, you bond with people.Ý Danielle and Kirsten came to my sweet sixteen party.Ý We lucked out they we were all out of the hospital at that time, because we were always in and out.ÝÝÝÝÝÝ Mother was a really good nurturing place, the staff spoke to you nicely and kindly, there was always someone there to listen to you. The doctors were great, it was the most like home of all the hospitals.Ý I was there six different times over four years. Thatís why I remember so much. My problems went very deep and it took so long to be where I am today.Ý I can honestly say if it wasnít for Mother and all the great therapists Iíve had, plus my family, I wouldnít be here today.î
Petra at Dangerfield State Psychiatric Center:
ÝÝÝÝ ìDangerfield was the worst of all the hospitals I
stayed in.Ý Right from the start the
staff was mean and just turned me off.Ý
The place was filled with dangerous kids, one claimed she sold weapons.
The staff was horrible.Ý The more I
wouldnít cooperate with them the harsher they became.Ý I wanted to leave and they started threatening me and making up
lies. I ended up confined to my room for days.Ý
Print this from my diary:
Dear Diary,
ÝÝÝ It is horrible ‚ awful.Ý I just stopped crying.Ý Today Lina told me if I left it would be AMA
and she called my parents and told them that.Ý
That made my mom nervous.Ý It
means they could commit me against my will.Ý
Then they had a team meeting.Ý
They said I had consequences ‚ either I could transition or stay in my
room, no radio, no books for 10 hours every day.Ý Lina was calling my mother to tell her not to take me home.Ý Lina laughed at me ‚THAT BITCH.Ý I told her she has no heart etc. Then she
said they were keeping me for an extended period of time.Ý I said, ìWeeks, months?Ý She didnít know. So I became
hysterical.Ý Elaine, the bitch came in
and talked to me and was mean and said I wasnít going home. So tough luck.Ý And then out of nowhere, with no merit
whatsoever, told me I havenít been eating and I still want to hurt myself.Ý I screamed, ìWHAT?îÝ I threw out my nasty tuna, so fucking what??Ý I eat like a pig and I donít want to hurt
myself.Ý So I signed a legal 72 hour
letter to get discharged and Iím praying I get out.Ý The problem is my parents.Ý
I know Lina must have talked them out of taking me home.Ý So what to do?Ý I also got yelled at and sent out of activity into my room for
comforting someone and refusing to drop asking what was wrong under theÝ staff director.Ý Fuck this shit.Ý 10 hours
a day in room, no CD player, no TV.Ý
This is a violation of right # 3. No reading materials, meals in the
room.Ý They are lying now, making up
stories to keep me here. Mocking me, laughing.Ý
I am so terrified of these people.Ý
I have been in my room almost all day.Ý
Iíve already signed myself out, they canít keep me here.Ý My mom called and I told her what they are
doing to me, she started crying and saying she didnít understand how they could
do this to me and they told my father they were just enforcing strict
consequences.Ý They have also been
telling my insurance person that I am extremely dangerous.Ý My mom and I know I am not! They are just
trying to dick me over.Ý So my mom was
so angry and said that on Friday, her and my father are signing me out.Ý They are saying Iím coming home with
them.Ý My mom told me to just keep my
calm and Iíll be out in 72 hours.Ý My
dad too.Ý Iím so grateful my parents are
supporting me.Ý God, I pray to you I am
safe and I need to go home!!!
After
I left Dangerfield, I wrote a letter to the state complaint board.Ý They violated many of my patient
rights
and they got investigated because of my letter!î
Petra at Rocky Stream University Hospital:
ÝÝÝÝ ìI was attending a special
private high school for girls with psychiatric and other problems when I wasnít
in the hospital.Ý This evil district
representative showed up at my parents house and said I had to be evaluated at
the Rocky Stream psych E.R.Ý It was so
scary.Ý It is a total locked unit,
everyone there is totally crazy!Ý This
girl with died black hair, you know the gothic look, came running at me
yelling, ìYou bitch, Iím going to kill you.îÝ
She was on a bad acid trip.Ý I
ended up having to have ECT, which that hospital supposedly has the best set up
for.Ý I donít remember a lot about that
hospital stay because the ECTÝ kills
some of your memory.Ý But I remember it
was a circular unit and it was big and you could get lost.Ý You were free to walk all over the
place.Ý And people ran rampant, some
really psychotic adults.Ý It was not a
safe place for teenagers.Ý I was 16 and
I was the youngest person there getting ECT.Ý
I donít really know if it made a difference because itís hard to
differentiate what happened. My mom seems to think it helped me a lot.Ý My psychiatrist didnít want me to do it. I
was fine with getting it, they had to have my permission to do it.Ý You have to have no food or drink for twenty
four hours, cause you could die. It was scary, but they show you a video of the
process.Ý You had to get into a hospital
gown in the morning and they take you in to do it, and I loved getting
anesthesia, I loved the doctor counting backwards and you would feel the waves
come over you and then you are out.Ý I
loved the feeling of going down, a total rest, no dreams, no nightmares. After
the procedure, I hated waking up, I was hysterically crying and screaming and
disoriented. I donít really know what they did. But itís very safe, not like
the olden days, itís very routine now. And itís weird the next treatment I had,
I woke up hysterically laughing. And supposedly this doctor who was renowned
for his expertise in ECT was treating me.Ý
Thatís why I ended up staying in Rocky Stream.Ý He was this famous guy and I thought he was an asshole. So before
they even put me under the anesthesia, I donít know where I got the balls to
say this to him but I said, ìYou know you think youíre such a big shot, youíre
such an asshole!î And all the nurses were gasping because here I am about to go
under anesthesia and get shock treatments from this guy.Ý They thought it was the funniest thing,
because he was on this big ego trip like ìIím Dr. Bigshot.î
Ý
Petra at Dragmont Childrenís Psychiatric Center:
ÝÝÝÝ ìAt one point I was sent to
Dragmont, I think we couldnít afford Mother at the time, you know the they were
very expensive and the insurance didnít cover everything. There were
people who were out of control, violent. There were these girls in Dragmont -
thank God I wasnít there when they did this - but I was on pass and I came back
from Christmas, and I found out these girls had plotted this whole thing to
escape, and they set a fire in the kitchen and they jumped the staff.Ý They attacked them, like some of them got
bit.Ý Thatís a dangerous job.Ý I knew this nurse Marianne and she was kind
of gruff but she was okay. This girl bragged about attacking her. I got really
mad at her and told her that was wrong.Ý
Marianne got really hurt, like with permanent damage.Ý I didnít like Dragmont at all.Ý They did not have enough therapy.Ý I had been through the process so many times
I knew how to demand more.Ý The step up
program was very punishing.Ý It wasnít
like Mother at all.Ý I didnít feel safe
there.Ý The only good thing I can say was
that my therapist, once I got her, was great and she did help me somewhat.Ý The whole place was very institutional and
they had to deal with real behavior problem kids and the staff was mostly
terrible.î
ÝÝÝÝ KIRSTEN
Kirsten is 21 years old.Ý She has been in and out of hospital from age 13-19.Ý She was an inpatient at the following hospitals:
- Mother Hospital in Port Hamilton ‚ Special Adolescent Unit
- Dragmont Childrenís State Psychiatric Hospital
- Rocky Stream University Hospital ‚ Psychiatric Unit
Kirsten was diagnosed with anorexia nervosa and mild depression.Ý Her eating disorder was severe and pervasive.
Ý
Kirsten in Mother Hospital:
ÝÝÝÝ ìI absolutely hated Mother hospital the
first time I went there.Ý I hated it
because my mom put me there.Ý My parents
couldnít deal with my dieting, which is what I called it at the time.Ý I had to travel down a long road before I
was able to admit I was an anorexic. My parents were always fighting with me.
My mother was a beast, she was the original mommy dearest.Ý We had the perfect house, the perfect
looking children, our rooms had to be perfect, we couldnít get less than
Aís.Ý I wanted to be a model. In
modeling you are encouraged to be thin, and they encouraged drug use to stay
thin. I am six feet tall and I weigh 135 pounds. I like myself now at this
weight. But once I was 79 pounds and I thought I wasnít thin enough.Ý With anorexia you literally starve yourself
to death. Iím Catholic and I even used to throw up the host from communion. I
still struggle today but I am so much better. I donít live at home anymore and
I still go to therapy every week.
ÝÝÝÝÝ Anyway, as I said I hated Mother
hospital at first. All those rules and regulations. I found it very invasive to
my rituals. They would never let me just be alone. They made me go sit at a
desk for an hour after eating, doing nothing while someone watched me, so I
wouldnít purge.Ý They monitored
everything I ate and kept careful watch on me all the time. They were trying to
help me.
ÝÝÝÝÝ They had this rubber room for you to go
scream in when you wanted to act out.Ý
Sometimes they would announce this code over the hospital loud speaker
ìMr. Powers, Mr. Powers!Ý Please come to
2 North.îÝ Which was a message for all
the manpower to come to the ward because someone was freaking out and going
crazy. And they would come and put the person in the rubber room.Ý You could flip out.Ý It was all kind of surrealistic. Seeing
people flip out and act weird.Ý It was
like being Dorothy in the Wizard of Oz.Ý
All of a sudden you are completely uprooted and in a weird place.Ý Some of itís friendly and supportive.Ý People want to help you find the way.Ý And some of it was as scary as the witches
castle.Ý It was after I went to Rocky
Stream that I really appreciated Mother and I began to let them help me.Ý They really were so nice to me even though I
was so hostile to them the first time I was there.Ý They didnít give up on me and they were strict, but not in a bad
way.
ÝÝÝÝÝ I met Danielle and Petra there.Ý Danielle was a very out of control girl and
I know she thought I was uppity.Ý She
just wasnít my type.Ý But Petra was my
anchor, she was a really good friend. They had lots of family therapy which was
great, it helped me free myself from my mother.Ý She had a tough time with this, but it helped her too.Ý Our relationship will never be perfect, but
itís improved a lot.Ý And with me being
out of the house now, things are much, much better.î
Kirsten at Dragmont Childrenís Psychiatric Center:
ÝÝÝÝ ìI ended up at Dragmont, I donít even remember why, I
think it was the insurance or maybe Mother had no beds.Ý Anyway,Ý
I hated that place.Ý There were a
lot of poor kids, kids from crack homes and really abusive homes.Ý They were scary and violent, always acting
out.Ý I hated the point system there,
they had more rules than a prison.Ý You
werenít treated as an individual, if one kid did something wrong the whole unit
got punished.Ý Then kids would get
violent towards each other.Ý One girl
almost beat up another one because we lost phone privileges. So instead of
learning to take responsibility for yourself you just hope that all the other
girls donít do something stupid.Ý
Everyone else has to do what they are supposed to so you can get a lip
gloss.Ý So that wasnít a fair place. The
food was disgusting!Ý Here I am with an
eating disorder and they want you to eat. It was made with really unhealthy
ingredients and most of it came from giant cans. Gross. It could make you want
to starve.Ý
ÝÝÝ Then this horrible thing happened. The
staff was mean, but this one guy, a staff aide, was really nice and would
listen to me and he was really cute. And then he hit on me!Ý And his wife worked there on another
unit.Ý He wanted me to meet him
somewhere when I got out on a pass, and I thought he was cute. ÝBut I realized it was dysfunctional and
wouldnít be a good idea. I knew it wasnít professional and normal.Ý Can you imagine how screwed up I would be if
I had an affair with this guy?Ý I told
my therapist but I didnít tell her his name, but she guessed it because an
accusation was made against him that this girl met him at a hotel and they had
sex.Ý She was 15. He was a scumbag and
it was passed over because they said she was crazy.Ý I had to go through this whole investigation.Ý He got suspended while the investigation was
going on.Ý And his wife worked on the
other unit and she was this big terrifying lady and here I am this skinny
anorexic. She would give me dirty looks and she was friends with the people on
my unit.Ý They already didnít like me so
this was another reason for them to hate me. The whole thing wasnít conducive
for me to get better.Ý Some of the staff
and my therapist all wanted to get me discharged because they knew this wasnít
healthy for me. It wasnít a safe environment.Ý
I have had as much trauma in the hospitals as I have had in my life!î
ÝÝÝÝ
Kirsten at Rocky Stream University Hospital:
ÝÝÝ ìThey didnít have enough
beds in Mother one time so I got sent to Rocky Stream Hospital. That was an
insane place.Ý I was with adults. I
never saw so many sick, demented people. There was this man who thought he was
Jesus and argued with another man who thought he was Satan.Ý Some lady went up to my mother and started
talking to her.Ý My mother had no idea
she was a patient.Ý And they were
talking all friendly small talk and she says to my mother, ìYes, I lost my
son.îÝ And my mother said , ìOh, Iím so
sorry.îÝ And she says to my mother,
ìYes, heís lost in the universe and they ate his penis.î I just loved that. The
look on my mothers face was so funny.
ÝÝÝÝ The unit was so huge, like a big circle.
It was like a prison, all locked up at night, but I really had the most freedom
here, but not in a good way.Ý You could
go around and around all day doing nothing.Ý
There were house phones on the walls everywhere. You would get paged on
the phone if they were looking for you.Ý
One time I got paged and while I was on the phone, I saw this man
standing outside my room running his finger over the number plate.Ý I had to go to the nurses station and when I
came back to my room, he was standing completely naked in front of the mirror
by the sink. He was holding my face powder compact open and he was scooping it
out with his fingers and eating it!Ý I
was only 15 at the time and this traumatized me.Ý I wanted to get out of there, I was hysterical. I called my Dad
and he called the head of the unit who said to him, ìOh weíve advised Mr. So
& So to not go in her room again.îÝ
Like that was supposed to make me feel safe!Ý So I didnít feel safe there at all.Ý
ÝÝÝÝ Then one night my mother called to see
how I was doing, she called the nurses unit and they told her not to panic but
they couldnít find me. What had happened was the night before it was really hot
in my room.Ý The lady who had the lost
son with the eaten penis had the room next to mine.Ý She was getting ECT, so I slept in her bed because it was too hot
in my room.Ý Her bed had all this
padding next to guard rails so she wouldnít fall out.Ý So they couldnít see me asleep behind the padding. They thought I
was lost.Ý Thatís what kind of close
observation they kept on me.Ý In Mother
they check on you every 15 minutes.î
ÝDANIELLE
Danielle is nineteen years old.Ý She has been in and out of hospitals from age 15-18.Ý She was an
inpatient at the following hospitals:
- Mother Hospital in Port Hamilton ‚ Special Adolescent Unit
- Birmington Hospital ‚ Psychiatric Unit
Danielle had a serious cocaine addiction and was also diagnosed with a mild bipolar disorder.Ý
Her behavior was often reckless and she described herself as a wild teenager.
Danielle in Mother Hospital:
ÝÝÝÝ ìI was fifteen and so into drugs and I
was this totally manic girl. Letís face it, I was wild. I was three years in
and out of Mother.Ý Thatís where I met
Petra and we became friends. I knew Kirsten too but she was such a fucking
princess. Oh sorry, are you gonna bleep out my curses?Ý Anyway, I felt Petra had a right to kill
herself, so once when she was on suicide watch, I smuggled her a tic tac box
that I stepped on and made sharp pieces.Ý
I passed it to her in a book. I was a crazy kid.Ý She used it on herself under the blanket and
the one-to-one nurse almost died when she found out.Ý Petra only hurt herself a little, it wasnít sharp enough to kill
her. I smuggled a shoelace and I helped her rig up this shoelace noose with a
chair, but it hurt her neck and didnít work.Ý
Later on we got found out and we lost all our privileges .
ÝÝÝÝ We were a coed unit at Mother, that was
pretty cool.Ý Most of the girls were
depressed, suicidal or into self mutilation. I was a drug addict and I just
wanted my junk.Ý My boyfriend would
visit me and pass me some coke.Ý They
caught on to him pretty quickly so he was banned from visiting, which really
sucked at the time.Ý Heís not my
boyfriend now, he really is a loser, he lives with a woman thirty years older,
sheís heís coke mamma and has eight dogs, itís really weird what drugs will
make you do.
ÝÝÝÝ But about Mother, lets just say I
rebelled at first and really acted out. It took me a while to agree to be
healed. They would not let you stay in your bedroom at all, you had to be busy
with activities and school all day. There was this boy who was really depressed
and he wouldnít get out of bed, so they pulled the mattress out into the hall
with him on it, because you absolutely could not stay in your room. They didnít
want you in a funk, they wanted to get you up and keep an eye on you if you
were depressed.Ý They were really
committed to making you better. I rebelled, but in the long run, this was the
best way they could have been. What can I say, they won me over, it really was
like a family.Ý It was work to get free
of my coke addiction, but even harder was dealing with all the issues after I
was clean.Ý I had a bipolar problem, but
itís very much under control now.Ý
ÝÝÝÝ My therapists were all great. They had
great group therapy, with a social worker.Ý
But she canít do that anymore because she spends all her time fighting
the insurance company. The biggest problem for me was getting kicked out
because the stupid insurance ran out. My Mom was fighting with the insurance
company all the time.Ý I would be let
out too soon, then pressures would build up and viola,Ý Iím baaaaack!Ý Thank God mostly my Mom got me back to Mother.î
Danielle at Birmington Hospital:
ÝÝÝÝ ìOne time when I overdosed I was taken to
Birmington. I was there for a month and a half, and it sucked. It was very
different from Mother. Because it was an adult unit and maybe there was only
one or two other teenagers there.Ý It
was very unstructured, you hardly had any therapy.Ý You had to be smart and know who to seek out to get therapy.Ý If you didnít fight for your time, you
wouldnít get therapy, or have anyone to talk to.Ý The head guy really pissed me off, he just didnít know how to
deal with me. Some staff were nice but they just didnít have time. Staff really
does make a difference, one guy, an aide, was really nice, he was so funny, he
called me Danielle from hell, because of my devil tattoo.Ý He made me laugh all the time.Ý Sometimes one person who cares can make a
difference.Ý But mostly that place was
for adults so they could care less about us.
ÝÝÝÝ You mainly watched TV all day. I got to
see a ton of videos. Nobody cared what you watched, you sat around, played
solitaire, you shuffled around, if you got visitors, fine.Ý You could go in your room, sleep all day,
but you mostly just wandered around.Ý
They didnít really know what was going on with us. The food was your
typical hospital crap, but at least you had a choice. They did do searches for
contraband and stuff, but if Petra and I had been in Birmington togetherÖoh
God, it scares me to think I would have successfully helped her commit suicide,
because with all that unsupervised time we would have found a way.Ý That would have been horrible.Ý What an asshole I was then.Ý Drugs make you into an asshole.Ý
ÝÝÝÝ So you could be depressed, and unless you
got therapy you could stay down for days, and no one would notice.Ý They had group therapy, but because they
didnít have any separate program for teenagers, you could be mixed with
anybody, even people who werenít psych patients but were depressed, like old
people.Ý Or they had Alzheimerís.Ý There was this old lady who was dying, it
was so depressing.Ý AndÝ this other lady was in her late 80ís. They
put her in the group and she thought we were her relatives and she was visiting
us for dinner. She was psychotic but it was from dementia or something.Ý She would say ìIím off to the hair dressers,
dear, it was nice chatting with you.î Or she thought she was the nurse and
sheíd say, ìNow off to bed honey, I have to do my rounds.î Or she would just
start singing, ìDaisy, DaisyÖîÝ It was
weird and hilarious at the same time. You could be with people who had really
horrible things happen.Ý It was
traumatic, but it was better than doing nothing.Ý I went back on drugs soon after I left there.î
ÝÝÝÝÝ BETH
ÝÝÝÝ Beth is fifteen years old and is the only one of the case studies still in the hospital.Ý She spent
her first month in:
- North Maple Psychiatric Hospital ‚ Psychiatric Unit
She is currently at:
- Dragmont Childrenís State Psychiatric Hospital
ÝÝÝÝ Beth suffers from obsessive-compulsive disorder. Her mother wanted the unique
manifestation of Bethís obsessive-compulsive behavior to be left out, keeping her anonymity.
She takes several medications to keep this under control, but has trouble staying focused or
staying still. Difficulties in interviewing effectuated her motherís filling in pertinent details.Ý I
combined their comments and put them in Bethís voice.Ý TV
Beth at North Maple Psychiatric Hospital:
ÝÝÝÝ ìNorth Maple has beautiful grounds. But
thatís about it.Ý It was stark and
sterile inside. Itís a total locked ward.Ý
I thought I was raped at North Maple by a man, one of the staff. It
turned out to be a psychotic episode.Ý
But I had to go through the whole rape kit and talk to the police.Ý They had to examine me. It was all so
horrible. I was so scared when I first got here.Ý I felt traumatized and nervous so it triggered this psychotic
thing.Ý I was hearing voices of the kids
from school, I thought they were talking about me all the time and I could hear
them.Ý I donít hear voices anymore.Ý Iím cured of that now.
ÝÝÝÝ They had a separate place for teenagers.
They had separate units, like they had a separate eating disorder unit.Ý I was there for acute care to be stabilized
and moved to Dragmont. They didnít have a lot of resources.Ý They had a lot of poor kids who were in and
out of foster care who had emotional problems. Once I was calmed down, it was
better. Mom liked the doctors and the nurses and staff and thought they were
pretty good for a state hospital. But the social worker sucked. I felt sick a
lot from the medications.Ý I was like an
experiment.Ý They were always giving me
tests and different drugs.Ý I donít
rememberÖI slept a lot, watched TV a lot.Ý
My Dad and Mom brought me lots of videos. The food was terrible. Before
I knew it, a month went by and I was sent to Dragmont.î
Beth at Dragmont Childrenís Psychiatric Center:
ÝÝÝÝ ìI hate it. It isnít helping me. I donít
understand why I have to stay there.Ý I
want to go home. This is like the army, they have million rules and some of the
kids are scary, they are tough and get violent. But I am more scared of some of
the staff. They are trashy, lower class, not very professional. One African
American aide made a racial remark against me. ìGirl you better stay out of my
koolaide, cause you donít know the flavor. Okay wonderbread?î Thatís not right
from a staff person, whoís supposed to be there to help you. But the white aide
is mean too.Ý Some are low class and
very mean.Ý This one very mean aide,
Audrey, has been abusing me since the day I got there.Ý She sayís I look too fat in my clothes.Ý She sayís Iím lazy, Iím not lazy, I have a
problem with my motor skills. She calls me a wet dog when my hair is wet. If
kids have hygiene problems she humiliates them in meetings. She thinks Iím
sloppy.Ý Itís not therapy when they look
down on you.Ý Most of them are bad,
except Sue is nice; she gives me my meds all the time. Sheís kind and has a
sense of humor.Ý She helps me in my
room.Ý Janet has a nice personality. She
runs the creative club I go to every Wednesday.Ý We write down our feelings in a book, we are doing an assignment,
ìWho Am I?îÝ The teachers of the classes
and therapists are nice itís the other staff people who are mean and terrible.
ÝÝÝÝÝÝÝ The first day I was here, I was
scared.Ý I was in the infirmary; they
asked me all kinds of questions.Ý They
searched my shoes; they searched my pockets for knives.Ý A lot of kids bring in weapons. They look
for contraband. Nobody told me how long I would be here.Ý They told me I would be here for
socialization, schooling and to help me with my OCD.Ý Itís very restrictive; I felt I wasnít going to make it.Ý There is no freedom.Ý After a while you just get used to it.Ý Do I feel safe? No, I feel I should be home.
ÝÝÝ They give me three different
medications.Ý I hate the side effects, I
gained a lot of weight and my face broke out really bad.Ý They told me about the side effects first,
so I was so scared to take the medicine.Ý
ÝÝÝÝ I go to school 9:30-3:30.Ý The teachers and classes are pretty
good.Ý I get group therapy on Mondays
from 4:00-5:00.Ý Itís good, but thatís
it, itís all the therapy I get. Itís not enough.Ý I feel I should have therapy every day.Ý Creative club and group, thatís all I do.Ý Group therapy is a bunch of girls talking
about their feelings.Ý They talk about
being sexually abused, some talk about drugs or their parents physically
abusing them.Ý The girls in my group are
age 12-18.Ý I like group.Ý
ÝÝÝÝ I donít like the way the building looks;
the whole place needs to be remodeled. And the place is very dreary with hard
plain furniture and bare walls. It has big brick walls, like prison walls.Ý They painted them pink for girls and blue
for the boys.Ý There is artwork, some
Picasso paintings. They need more colorful art on the walls. I have a closet
and drawers for my stuff. But they need more nice furniture. They let you bring
your own blanket and stuffed toys from home, but I get searched every time I go
home on a pass.Ý Plus they do room
searches. Only one to a bathroom at a time. Ten of us share a bathroom. No
boys. There is three or six in a room.Ý
I have two roommates: Estelle was raped by her father and Marissa slit
her wrists. All the girls here are a lot sicker than me; I donít understand why
I am here. I donít act out, or get violent; I donít take drugs or have
sex.Ý I donít self-harm or harm
others.Ý I didnít do anything bad.
ÝÝÝÝ The food is terrible; itís all fattening
canned stuff that tastes so bad. Itís thrown together and barely edible. The
staff will have a really nice steak dinner and they donít share it with the
kids. My medication makes me gain weight, and then I have to eat this
fattening, canned, institutional food.
ÝÝÝÝ There are a lot of bad kids here.Ý When they get violent, they get a needle and
they go in the seclusion room.Ý Bad is
acting out, screaming at the staff, using contraband or if they find
drugs.Ý If I had talked back to Audrey,
they would have put me on ITL.Ý They
take away privileges like TV. You canít go to activities.Ý So you have to take it when the staff are
mean, cause they have all the power.Ý
The point system isnít fair.Ý
They make it hard and very uncomfortable to ask for things you need or
complain about anything.Ý
ÝÝÝÝ We do tons of chores.Ý We do all the cleaning.Ý Mop the bathroom floor, clean the linen
closet, clean the kitchen.Ý If you are
on the highest level, they will pay you something for it.Ý They donít have big cleaning staff so the
kids do the cleaning.Ý This is not like
home; itís like a prison.Ý You are under
constant supervision.Ý You can only wear
makeup on full privilege. You start out at the lowest level and you are there
for a while.Ý You have to do your own
laundry.Ý You have to work.Ý If a kid is depressed and canít get out of
bed, they rip the covers off and say, ìGET UP! Two hundred negatives!îÝ If you get negative points up to 1000 you go
on ITL.Ý I was put on ITL for losing my
card three times.Ý Itís a paper we write
on.
ÝÝÝÝ They do have a lot of activities.Ý They have baseball, volleyball, swimming,
table games, full privilege table games, sewing, reading, art, creative
therapy, rollerblading.Ý They make all
the boys put on roller blades and skate around and around the gym to get their
aggression out.Ý You can use the
computer, they have TV, you are allowed your own CD players and music if you
are on level two.Ý To get a lot of the
stuff you have to be level 2 or higher, but itís really hard to get to level 2.
We hardly get to go out.Ý Everything is
inside.
ÝÝÝÝ The worst thing that made me cry was not
being able to go home one weekend because I was on ITL. I hardly get to see my
family as it is. I miss my family so much.Ý
Family can only visit once a week. They donít want any visitors during
the week and donít let anyone else visit.Ý
The first ten days no one is allowed to visit you at all.Ý Those were the worst ten days.Ý I am only allowed to call home on Tuesday
and Thursday night.Ý Some of the kids
come from really bad homes, so itís actually better for them, but not for
me.Ý
ÝÝÝÝÝ I also hate it when I have to see kids
go in the seclusion room when they flip out. A kid threw a chair through a
glass window. Bad things happen. This girl was saying that another girl forced
herself sexually on her. They called my mom to ask if it was okay for me to be
a witness.Ý Mom said no, because she didnít
want anything upsetting me, besides I didnít see anything.Ý A lot of that stuff happens here.î
Analysis of the Interviews:
ÝÝÝÝ To make sense of the interview data, I created a rating chart to organize and clarify the girls
perceptions of the six hospitals.Ý I chose criteria from: the home survey, my study of the
psychopathologies and the professional and case study interview material.ÝÝ
ÝÝÝÝ
ÝÝÝÝ JAlways/ExcellentÝÝÝÝÝÝÝÝÝÝÝÝ KSometimes/FairÝÝÝÝÝÝÝÝÝÝÝÝÝÝ LNever/PoorÝÝÝÝÝÝÝÝÝÝÝÝÝÝ N/A not applicableÝÝÝÝÝÝ
|
|
Mother |
Dangerfield |
Birmington |
Dragmont |
Rocky Stream |
North Maple |
|
Was the
staff friendly, caring, kind, supportive, respectful? |
J |
L |
K |
L |
K |
J |
|
Did you
feel you had enough therapy? |
J |
L |
L |
L |
L |
L |
|
Did you
have individual therapy? |
J |
L |
L |
K |
K |
J |
|
Did you
have group therapy? |
J |
K |
K |
J |
K |
K |
|
Did you
have family therapy? |
J |
L |
L |
L |
L |
L |
|
Did you
have a variety of mental and physical activities to do? |
J |
K |
L |
J |
L |
L |
|
Was
there a point system? |
J |
J |
L |
J |
L |
L |
|
Did you
think the point system was fair? |
J |
L |
N/A |
L |
N/A |
N/A |
|
Was the
hospital equipped to handle your particular illness? |
J |
L |
L |
K |
L |
K |
|
How did
you feel overall about the other kids? |
J |
L |
K |
L |
L |
K |
|
Were
you allowed frequent visits from your family? |
J |
L |
J |
L |
K |
K |
|
Did you
feel you had someone you could confide in? |
J |
L |
L |
K |
L |
L |
|
Were you
allowed frequent visits from your girlfriends? |
J |
L |
J |
L |
L |
L |
|
Did you
feel safe and secure in this hospital? |
J |
L |
L |
L |
L |
L |
|
Did you
feel you had privacy from other patients? |
J |
L |
J |
L |
L |
L |
|
Were you
allowed visits from your boyfriend? |
J |
L |
J |
L |
L |
L |
|
Did you
have good tasting, quality food? |
K |
L |
L |
L |
L |
L |
|
Did you
have a nice place to take a shower/bath? |
J |
K |
K |
K |
K |
K |
|
Could you
have a walkman or listen to your own CD's? |
K |
K |
J |
J |
J |
J |
|
Were
you allowed to use the telephone regularly? |
J |
L |
J |
L |
J |
L |
|
Did you
feel like you belonged, fit in? |
J |
L |
L |
L |
L |
L |
Fig. 3
ÝÝÝÝ I expected tales of sterile decor and plain walls.Ý I expected complaints about restrictions and
lack of freedom and privacy.Ý What I didnít expect was that the girls donít feel safe, donít always
have a quality staff, may suffer abuse from staff or feel threatened by other patients, donít get
enough therapy, donít have enough activities, have no one to confide in and feel they donít fit it.Ý
Adults are mixed with adolescents and families are sometimes left out. And yes, the food is
terrible.Ý My home elements of safety/security, comfort and sense of belonging are blatantly
lacking in most of the hospitals except for Mother hospital!
ÝÝÝÝ The egregious lack of safety tops the list.Ý All four of the girls had episodes of feeling unsafe.Ý
The unprofessional, ìlow classî or punitively oriented staff contributed to this. The verbal abuses
towards Beth, sexual harassment of Kirsten or overly punitive reactions to Petra in Dangerfield
shouldnít be tolerated, period.Ý Mixing of adolescents with adults and mixing of violent/behavior
patients with other psychopathologies sets the scene for safety issues.Ý The argument for
segregation based on age and psychopathology surfaces again. Some of the more frightening
experiences, like Kirstenís encounter with the naked makeup eating man, occurred because
teenagers donít always have separate wards. The university hospital has a psychiatric childrenís
ward up to age thirteen and an adult ward.Ý The adolescent is overlooked even by renowned
hospitals. Placing anxiety riddled teens like Beth in with teens who commit violent acts
predisposes her to more anxiety as a captive witness.Ý Understanding the various different
conditions and severity of patients illness needs exploration to improve treatment. (Leon, 2000.)Ý
Also, lack of supervised activities leaves teenagers open to all kinds of trouble, especially for the
suicide patient, drug abuser or anorexic. I think about Petra, Kirsten and Danielle wandering
around for hours like stray cats, unsupervised and ignored.
ÝÝÝÝ Would anyone ever think of psychiatric hospitals as not providing enough therapy?Ý This
surprised me more than anything since inpatient hospitalization fundamentally should focus
efforts on healing the patient through therapy.Ý Are therapies lacking because of poor resources?Ý
I would think other amenities would suffer before therapy would.Ý
ÝÝÝÝ Families are the number one priority of our teens and yet not all the hospitals allowed for
visits or offered family therapy.Ý Dragmont actually barred parents from the first ten days of
treatment.Ý Is this because the majority of the patient population came from abusive families?
The girls rated most of the hospitals as not giving them a sense of belonging.Ý If families are not
included and a surrogate family is not created, our patients are sure to feel isolated and lonely.
Feelings not conducive to healing.Ý
ÝÝÝÝ In 1992, Louise Armstrong wrote And They Call It Help, an expose of psychiatric hospitalÝÝ
treatment for children and adolescents.Ý She found similar issues with unqualified staff, therapies
not providedÝ and punitive restrictions.Ý Why almost ten years later do we still have the same
problem?Ý Why are the hospitals so lacking?ÝÝÝÝ
HOME-MORE OR HOME-LESS: THE PSYCHIATRIC HOSPITALS
ÝÝÝÝÝÝ My attempt to keep this study well rounded has its restrictions.Ý I was routinely and
irrevocably denied access to psychiatric wards, a policy strictly enforced to protect patient
privacy from uninvited guests.Ý I took this graciously but I didnít appreciate the flat refusals for
interviews via telephone or ignored phone calls. No pretense worked; hospitals did not want to
comment.Ý I wanted to give administrators equal time, but such is the plight of a researcher:
denial of some pieces of the puzzle.Ý The only exception: Mother Hospitalís Nurse Janet Cooper
generously granted me a telephone interview and offered me printed materials normally given to
parents.
ÝÝÝÝ Undaunted, I hunted down some statistics on the hospitals to look for connections to
the lack of home elements:
|
Hospitals |
Type of Facility |
Number of Beds |
Predominant Psychopathology* |
Neighborhood Location* |
|
Mother Hospital |
Private Hospital-Separate
Psychiatric Units for Adults and Adolescents. |
10 |
Affective Disorders Eating Disorders Psychiatric Trauma |
Upper Income Suburban |
Dangerfield PsychiatricHospital |
State Run Facility For Children under 18 (wards of the state reside here). |
50 |
Behavioral-Violence Schizophrenia Psychotic Disorders |
Lower Income Suburban |
Birmington Hospital |
Private Hospital- Separate
Psychiatric Unit No Children under 13 Adolescents treated w/Adults |
21 |
Affective Disorders Anxiety Disorders |
Upper Income Suburban |
|
Dragmont Children's Psychiatric
Hospital |
State Run Facility For Children Under 18 |
69 |
Behavioral-ViolenceÝÝÝÝÝÝÝÝÝÝÝ |
Middle Income Suburban |
|
Rocky Stream University Hospital |
University Hospital Separate Psychiatric Units for Children
5-13 Adolescents treated w/Adults |
40 |
Variable/Many patients referred
for Intensive ECT |
Upper Income Suburban |
|
North Maple Psychiatric Hospital |
State Run Facility Separate small units for
Children/Adolescents Most beds for Adults. |
200 |
Behavioral-Violence Psychiatric Trauma Schizophrenia Psychotic Disorders |
Middle Income Suburban |
Fig.
4ÝÝ *Data is based on case study, staff or
parent observation. All other statistics are courtesy ofÝ Newsday online.
ÝÝÝÝ Obvious influencing variables are private vs. state hospitals, separate adolescent units vs.
adolescent/adult units and few vs. many beds.ÝÝ Private hospitals like Birmington have more
resources, but if spending doesnít include specialized units and treatment plans, what good does
it do our teenager?Ý North Maple rated excellent for their staff even though they lacked resources
for programming.Ý This challenges the argument that you need resources to produce quality
staffing.Ý North Mapleís success, in this one area, may lie more in good management and their
philosophy of staff to patient relationship; too bad they couldnít provide much else.Ý Rocky
Streamís lack of an adolescent unit surprised me.Ý I thought a university teaching hospital would
offer a wide scope of treatment programs.
ÝÝÝÝ Economic demographics shows no influence on hospital ratings in this study.Ý Hospitals
received poor ratings regardless of upper, middle or lower income locations.Ý The demographics
however, may affect the type of psychopathology treated.Ý Middle and lower incomes hospitals
above, have a predominance of behavior/violence issues.Ý I empathize with staff in dealing with
this difficult and dangerous patient population.Ý I refer back to Petraís recount of Marianne, the
staff member attacked and bitten while the kitchen was set on fire in Dragmont.Ý Even
the most loving and conscientious of workers would sour after continual exposure to this.ÝÝ
State hospitals and large facilities tend to focus on controlling behavior. (Almond, 1974)Ý
Dragmont and Dangerfield are both state run, under age 18 facilities, dealing with issues of
violent behavior. This explains the reason for the punitive point system and restrictions used to
maintain order.Ý These teens are not criminals, they have a psychopathological cause for their
behavior, but should patients like Beth, Petra and Kirsten be treated in the same kind of
environment?Ý Researchers and psychiatric professionals alike show interest in matching patients
to separate treatment environments to improve the outcome of their therapy.Ý (Walsh, Craik &
Price, 2000)Ý Only trial studies measuring treatment outcomes will prove the point.Ý
ÝÝÝÝ My lack of information from hospital administrators and staff of the five deficient hospitals,
hinders my ability to answer for them.Ý
Mother
Hospital ‚ a model for home in the hospital
ëëIt was the most like home, the staff was nurturing, nice, kind.Ý They really listened to you.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Petra,
ìThey didnít give up on me.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Kirsten
ìThey were committed to making you better. It really was like family.î
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ -Danielle
ÝÝÝÝ The best argument for the value of home in the hospital is Mother hospital, a model for
creating the therapeutic environment for teenage girls.Ý
The secrets of their success lies in:
-private hospital/available resources
-professional staff who truly cares for the patient, will listen and be a confidante
-small number of beds puts an ideal staff to patient ratio
-full spectrum of frequent therapy provided: individual, group and family
-individualized treatment plans
-full involvement and visiting rights for family, keeping them educated and well informed
-full program of activities and quality schooling
-safety, comfort and privacy in a pleasant environment
ÝÝÝÝ Mother received an almost perfect score.Ý A little more effort in food preparation and lighter
restriction on CD players are all thatís needed to make this a utopia of hospitals for Petra, Kirsten
and Danielle. The most poignant quote comes from Petra:
ìIf it werenít for Mother HospitalÖI wouldnít be here today.î

Beautiful outdoor garden and
atrium area of Mother Hospital.
Buildings can convey
subliminal messages as to how the patient
is perceived by the hospital.
(Lennard & Gralnick, 1986)
HOMEWARD
BOUND ‚ CONCLUSION
ÝÝÝÝ Over the last thirty years, the number of patients hospitalized in three of Long Island state run
psychiatric hospitals, declined from 33,000 to 2,300. State hospitals are receiving limited funds
as community based support systems increase. (Newsday, 1999)Ý Inpatient care ranks as the
highest expense of mental health treatment. (Mechanic, McAlpine & Olfson, 1998) Economics plays a role in the
decision of placing an adolescent in the hospital.Ý Insurance company pressure might not make it
the treatment of choice. (Blanz & Schmidt, 2000)Ý Dr. Tonla brought out the issues of managed care to
shorten hospital stays and reminds us ìhospitals are in the
business of making money first.î
ÝÝÝÝ Looking at all these factors plus the inadequacies I discovered in this sampling of hospitals
might lead me to abandon my search and hope for home in the hospital.Ý Why should anyone
bother improving programs with nurturing elements of home, if limited by resources and time?Ý
The shift toward more outpatient vs. inpatient therapy places our teenager in the hospital for
short intensive stays followed up by outpatient services.Ý This is less expensive and restrictive,
but there is no proof yet that this is an effective solution. (Blanz & Schmidt, 2000)Ý As with the girls in this
study, many inpatient adolescents have multiple psychopathologies increasing the seriousness of
their illness. Outpatient services arenít adequate to help the more severe cases.Ý Most inpatients
have already tried outpatient therapy without success. (Blanz & Schmidt, 2000)Ý Hospitalization is still very
necessary, so I champion the cause of home in the hospital.
ÝÝÝÝÝ Hospital budget administrators need to look towards the forgotten adolescent and offer
resources for improving programs.Ý I suggest sensitivity training and education for all levels of
personnel to improve staff quality, especially with safety issues.Ý This can be done ìin houseî to
cut costs.Ý Families absolutely have to be part of the process, open communication costs nothing
but time.Ý If therapy is not a priority, why bother at all?Ý Hospitals must support this.Ý
ÝÝÝÝ I realize my research is limited to a small corner of the psychiatric hospital world, examining
a tiny demographic by a researcher without a psychiatric background.Ý I challenge others to pick
up the cause to look for abuses, deficits and solutions to the problem.Ý Identify model hospitals
and examine them for patient outcomes which may serve to change the mind of managed
care to spend less on wasted outpatient services for the seriously ill teenager and more on quality
inpatient care.
ÝÝÝÝ Indulge a humble researcher in creating a fantasy hospital.Ý If I were in the drivers seat and
money were no option I would create a world of healing:
Ý A small hospital complex on beautiful grounds, near a mountain or
lake, with gardens and waterfalls.Ý The
complex includes a main building surrounded by individual little cottages.Ý These would serve as small group homes,
keeping adolescents with similar illnesses togetherÝ The house would be fully staffed with nurses, aides and a
professional cook.Ý The main hospital
offers all traditional medical, individual, group and family therapies plus
alternative healing therapies i.e. mind/body techniques, massage therapy, light
and aroma therapy.Ý Activities would be
abundant and varied, with emphasis on outdoor physical exercise and sports,
cognitive problem solving with puzzles and games, art and music classes, yoga,
pet therapy and gardening.Ý All emphasis
would be on building self esteem and healing the body, mind and soul.Ý
ÝÝÝÝ I am not in the drivers seat. Managed care is driving the car, and the hospital budget
administrator is in the passenger seat.Ý A teenage girl, named Beth, is in the back seat.Ý They drive
her to an unknown destination.Ý I pray for a safe journey home.
ÝÝÝÝ Is valuing home in the hospital worthwhile?Ý For my answer, I have only to look in the eyes
of three beautiful, young, healthy girls: Petra, Kirsten and Danielle.
ÝÝÝÝ
ÝÝÝÝÝ
BIBLIOGRAPHY
Almond, R.Ý (1974).Ý The healing community.Ý New York:Ý Aronson.
Altman, I. & Werner, C. M.Ý ed.Ý (1985).Ý Home environments.Ý New York:Ý Plenum.
Armstrong, L.Ý (1993).Ý And they call it help: The psychiatric policing of americaísÝÝÝÝ
ÝÝÝÝ children.Ý New York:Ý Addison-Wesley.
Berger, L., & Vuckivic,
A., M.D.Ý (1994).Ý Under observation: Life inside a
ÝÝÝÝ psychiatric hospital.Ý New York:Ý Tichnor.
Blanz, B., & Schmidt, M. H.Ý (2000).Ý Practitioner review: Preconditions and
ÝÝÝÝ outcome of inpatient treatment in child
and adolescent psychiatry.Ý Journal
of Child
ÝÝÝÝ Psychology and Psychiatry, 41,Ý 703-712.
Brooks-Gunn, J., Ph.D. & H. Foster, W. H., Ph.D.Ý (2000).Ý Literature review on theÝÝ
ÝÝÝÝ effectiveness of youth development programs in substance abuse prevention.Ý Grant
ÝÝÝÝ Results Report: Robert Woods Johnson Foundation.Ý Retrieved March 8, 2001 from the
ÝÝÝÝ World Wide Web: http://www.rwjf.org/health/032701s.htm.
Brooks-Gunn, J., Ph.D. &
H. Foster, W. H., Ph.D.Ý (2000).Ý Teachers college, columbia
ÝÝÝÝ university, center for young children and families.Ý Grant Results Report: Robert Woods
ÝÝÝÝ Johnson Foundation.Ý Retrieved March 8, 2001 from the World Wide Web:
ÝÝÝÝ http://www.rwjf.org/health/032701s.htm.
Boyd-Franklin, N., & Hafer Bry, B.Ý (2000).Ý Reaching out in family therapy.Ý
ÝÝÝÝ New York:Ý Guilford.
Carroll, L.Ý (1971).Ý Alice in wonderland.Ý New York:Ý Norton.
Chiles, J., M.D.Ý (1986).Ý The encyclopedia of psychoactive drugs: Teenage depression andÝÝ
ÝÝÝÝ suicide.Ý New York:Ý Chelsea House.
Cooper Marcus, C.Ý (1995).Ý House as a mirror of self.Ý Berkeley:Ý Conari.
Frankel, B., Ph.D., &Ý Kranz, R.Ý (1994).Ý Straight talk aboutÖteenage suicide.ÝÝÝÝÝÝ
ÝÝÝÝ New York:Ý Facts on File.Ý
Geldard, K., & Geldard, D.Ý (1999).Ý Counselling adolescents.Ý London:Ý Sage.
Gottesfeld, H., Ph.D.Ý (1977).Ý Alternatives to psychiatric hospitalization.Ý New York:ÝÝÝ
ÝÝÝÝ Gardner.
Gould, M. S., Wallenstein, S., & Kleinman, M.Ý (1990).Ý Timeclustering of teenage suicide.Ý
ÝÝÝÝ American Journal of Epidemiology, 131, 71-78.
Govig, S. D.Ý (1994).Ý Souls are made of endurance:Ý Surviving mental illness in the
ÝÝÝÝ family.Ý Louisville, Kentucky:Ý Westminster John Knox.
Gralnick, A.Ý (1975).Ý Humanizing the psychiatric hospital.Ý New York:Ý The Gralnick
ÝÝÝÝ Foundation.
Karp, D. A. & Tanarugsachock, V.Ý (2000).Ý Mental Illness, Caregiving, and Emotion
ÝÝÝÝ Management.Ý Qualitative Health Research, 10(1).Ý 6-25.
Kaysen, S.Ý (1993).Ý Girl, interrupted.Ý New York:Ý Turtle Bay.
Kennedy,
J., & McCarthy, C. J.Ý (1998).Ý Bridging worlds: Understanding and
ÝÝÝÝ facilitating adolescent recovery from the trauma of abuse.Ý New York:Ý Haworth.
ÝKhan, A. U., M.D.Ý (1990).Ý Short-term psychiatric hospitalization of adolescents.Ý
ÝÝÝÝ Chicago:Ý Year Book Medical.
Korpell, H. S., M.D.Ý (1994).Ý How you can help: A guide for families of psychiatric
ÝÝÝÝ hospital patients.Ý Washington D.C.:Ý American Psychiatric.
Leon S. C.,Ý B.A.,Ý Lyons, J. S., Ph.D.,Ý & Uziel-Miller, N. D., B.S.Ý (2000).Ý
ÝÝÝÝ Variations in the clinical presentation of children and adolescents at eight psychiatric
ÝÝÝÝ hospitals.Ý Psychiatric Services, 51,Ý 786-790.
Lennard,
H. L., Ph.D., & Gralnick, A., M.D.Ý
(1986).Ý The psychiatric
hospital:ÝÝÝ
ÝÝÝÝ Context, values, and therapeutic process.Ý New York:Ý Human Sciences.
Masters, K. J.Ý (1997).Ý Using a coordinated treatment system to minimize child psychiatric
ÝÝÝÝ hospitalization.Ý Journal of the American Academy of Child and Adolescent Psychiatry, 36,
ÝÝÝÝ 566-568.
Mechanic, D., McAlpine, D. D., & Olfson, M.Ý (1998).Ý Changing patterns of psychiatric inpatient
ÝÝÝÝ care in the United States, 1998-1994.Ý Archives of General Psychiatry, 55, 785-791.
Minuchin,
S., Rosman, B. L., & Baker, L.Ý
(1978).Ý Psychosomatic
families: Anorexia nervosa inÝÝÝ
ÝÝÝÝ context.ÝÝÝ Cambridge, Ma.:Ý Harvard.
Mohr, W. K.Ý (2000).Ý Rethinking professional attitudes in mental health settings.
ÝÝÝÝ Qualitative Health Research, 10,Ý 595-611.
Newsday/Long Island A to ZÝ (1999).Ý Psychiatric hospitals.Ý Retrieved February 27, 2001, fromÝÝÝ
ÝÝÝÝ the World Wide Web: http//www.newsday.com/az/bhpsych.htm.
North County Psychiatric Associates.Ý (2001).Ý Cartoon of managed health care.Ý Retrieved April 19,
ÝÝÝÝ 2001, from the World Wide Web: http//www.hmopage.org/images/hmo.gif.
Olds, A. R.Ý (1978).Ý Psychological considerations in humanizing the physical environment
ÝÝÝÝ of pediatric outpatient and hospital settings. In E. Gellert
(Ed.),Ý Psychological aspects
ÝÝÝÝ of pediatric care.Ý (pp. 111-131).Ý New York:Ý Grune & Stratton.
Parrott III, L., M.D.Ý (2000).Ý
Helping the struggling adolescent: A guide to thirty-six
ÝÝÝÝ common problems for counselors, pastors, and youth workers.Ý Michigan:Ý
Zondervan.
Pipher, M., Ph.D.Ý (1994).Ý Reviving ophelia: Saving the selves of adolescent girls.Ý
ÝÝÝÝ New York:Ý Ballantine.
Piserchia, E. A., Bragg, C. F., & Alvarez, M. M.Ý (1982).Ý Play and play areas for
ÝÝÝÝ hospitalized children.Ý Childrenís Health Care. 10(4).Ý 135-138.
Pluterbaugh, D.Ý (1999).Ý Lifestyle assessment and changes: Using the healthy lifestyle
ÝÝÝÝ worksheet in practice.Ý Psychiatric Rehabilitation Journal, 23(1).Ý 70-74.
Rybczynski, W.Ý (1986).Ý Home: a short history of an idea.Ý New York:Ý Penguin.
Schoen Johnson, B.Ý (1995).Ý Child, adolescent & family psychiatric nursing.Ý
ÝÝÝÝ Philadelphia:Ý Lippincott.
Sharkey, J.Ý (1994).Ý
Bedlam: Greed, profiteering, and fraud in a mental health system gone
ÝÝÝÝ crazy.Ý New York:Ý St. Martinís Press.Ý
Squire, M. B., Stout, C.E., & Ruben, D.H.Ý (1993).Ý Current advances in inpatient
ÝÝÝÝ psychiatric care: A handbook.Ý Westport, Ct.:Ý Greenwood.
Steiner, H., & Yalom, I. D.Ý ed.Ý (1996).Ý Treating adolescents.Ý San Francisco:Ý Jossey-
ÝÝÝÝ Bass.
Supeene, S. L.Ý (1990).Ý
As for the sky, falling: A critical look at psychiatry and
ÝÝÝ suffering.Ý Toronto:Ý Second Story.
Thompson
Proust, H., &Ý D.T. (1999).Ý Counseling and psychotherapy with
ÝÝÝÝ children and adolescents: Theory and practice for school and clinical settings.Ý 3rd ed.Ý New
ÝÝÝÝ York:Ý Wiley.
Walsh, Bruce, W., Craik, K. H., &. Price, R. H., ed.Ý (2000).Ý Person-environment
ÝÝÝÝ psychology: New directions and perspectives.Ý 2nd ed.Ý New Jersey:Ý Erlbaum.
Warner, R., M.D., D.P.M., ed.Ý (1995).Ý Alternatives to the hospital for acute psychiatric
ÝÝÝÝ treatment.Ý Washington, DC:Ý American Psychiatric.
ATTACHMENTS
1.
SURVEY OF HOME

What is your first name (no last name)?
E-mail address?
How old are you?
What kind of house/apartment do you live in?Ý Describe it and also draw a picture if you
want to:
What do you like best about your home?Ý Think about what makes you feel good.
What sights do you like?
What sounds do you like?
What smells do you like?
What tastes do you like?
What do you like to touch, what feels good to your
hands?Ý
Do you have any plants?Ý Do you like having plants?
Do you have pets?Ý
Do you like having pets?
Do you have privacy in your home?
Do you feel comfortable in your home?
Do you feel safe and snug in your home?
Describe your room.Ý
What do keep in your room? How is it decorated?Ý Write about it and include a picture if you
want to.
What else would you add to your room if you could?
How many people are in your family?Ý How do you feel about your family?
Have you ever been away from home?Ý For what reason and how did it make you
feel?
Have you ever been in the hospital over night?Ý How did it make you feel?
Did you ever visit anyone in the hospital?Ý What did you think of it?
Here is a list of 30
things from HOME.Ý Hereís what you do:
READ THE WHOLE LIST
v
Put numbers next to each thing in order of
importance.
v
The most important would be number 1, then 2 and so
on.
v
If you donít think itís important cross it off the
list.
v
You may add things you think are important.
___Sleeping in a comfortable bedÝÝÝÝÝÝÝ ___Playing on the computerÝÝÝÝÝÝÝÝÝÝÝ
___Wearing favorite clothesÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Eating junk food
___Watching television/videosÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having art/decorationsÝÝÝÝÝÝÝ
___Eating home cooked mealsÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Feeling safe/secureÝÝÝÝÝÝÝ
___Reading favorite booksÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having a cozy chair/couchÝÝÝÝÝ
Ý
___Spending time with your familyÝÝÝÝÝÝÝ ___Having leisure time
Ý___Having
plants/flowers/gardenÝÝÝÝÝÝÝÝÝ
___Wearing cosmeticsÝÝÝÝÝÝÝÝÝÝÝ
ÝÝÝÝÝÝÝ
___Personal stuff from your roomÝÝ ÝÝÝÝÝ ___Listening
to your CDísÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ
___Exercising/playing sportsÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having privacy
___Spending time with girlfriendsÝÝÝÝÝÝÝÝ ___Talking on the telephoneÝÝÝÝÝÝÝÝÝÝ
___Taking a warm bath or showerÝÝÝÝÝÝÝÝ ___Playing video games
___Playing with your petsÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having someone to confide in
___Celebrating birthdays/holidaysÝÝÝÝÝ ___Studying at your own desk
___Having enough drawer/closet spaceÝÝÝ ___Having freedom to go out
Ý___Spending
time with a boyfriendÝÝÝÝ ___Feeling
like you belong/fit in
Pretend you are going into the hospital for a few
months to a year!
WHICH THINGS FROM HOME WOULD YOU WANT WHILE IN THE
HOSPITAL? Remember there are no wrong or silly answers, if you think
it's important it is!
ÝÝÝÝ READ THE
WHOLE LIST
v
Put numbers next to each thing in order of
importance.
v
The most important would be number 1, then 2 and so
on.
v
If you donít think itís important cross it off the
list.
v
You may add things you think are important.
___Sleeping in a comfortable bedÝÝÝÝÝÝÝ ___Playing on the computerÝÝÝÝÝÝÝÝÝÝÝ
___Wearing favorite clothesÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Eating junk food
___Watching television/videosÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having art/decorationsÝÝÝÝÝÝÝ
___Eating home cooked mealsÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Feeling safe/secureÝÝÝÝÝÝÝ
___Reading favorite booksÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having a cozy chair/couchÝÝÝÝÝ
Ý
___Spending time with your familyÝÝÝÝÝÝÝ ___Having leisure time
Ý___Having
plants/flowers/gardenÝÝÝÝÝÝÝÝÝ
___Wearing cosmeticsÝÝÝÝÝÝÝÝÝÝÝ
ÝÝÝÝÝÝÝ
___Personal stuff from your roomÝÝ ÝÝÝÝÝ
___Listening to your CDísÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ
___Having exercising/sports equipment ___Having
privacy
___Spending time with girlfriendsÝÝÝÝÝÝÝÝ ___Talking on the telephoneÝÝÝÝÝÝÝÝÝÝ
___Taking a warm bath or showerÝÝÝÝÝÝÝÝ ___Playing video games
___Playing with your petsÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ ___Having someone to confide in
___Celebrating birthdays/holidaysÝÝÝÝÝÝ ___Studying at your own desk
___Having enough drawer/closet spaceÝÝÝ ___Having freedom to go out
Ý___Spending
time with a boyfriendÝÝÝÝ ___Feeling
like you belong/fit in
ÝTHATíS IT,
YOUíRE DONE!
THANKS FOR BEING PART OF MY RESEARCH FOR SCHOOL.
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ PEACE AND
HAPPINESS,
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ
ÝÝÝÝ ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝJANE (A
REAL HOMEGIRL)
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ
E-mail:Ý jasmina@excite.com
Ý
APPENDIX
IÝÝÝÝÝ OBJECT OF AFFECTION (INFECTION)
IIÝÝÝÝ HOUSE OF PAIN
IIIÝÝ BEAUTY AND THE BEASTIE BOYS
IVÝÝ DONíT TRY THIS AT HOME
Jane Schreck ‚ WWII ‚ 2/7/01
Objects of Affection (Infection)ÝÝ
ÝÝÝÝ Joseph is eighty-one years old.Ý On the surface he is white, Irish, Catholic, Republican, father of eight, grandfather of eight, retired corporation employee, ivy school grad, war vet, suburban home owner and by outward appearances your ìregular cup of Joeî.Ý These labels can hint at influences and some stereotypical behaviors but so much of Josephís psyche is revealed when you take a metaphorical look at three ordinary yet highly significant belongings: a red sweater vest, wooden rosary beads and a black logbook.
ÝÝÝÝ The red sweater vest is old, pilled, faded, worn and still considered ìwearableî by the owner, an arguable point to his relatives.Ý He wears it almost every day, pausing only to launder it occasionally.Ý We all have those clothes that are so comfortable by our own definition, items that soften and ìbreak inî with age and mold themselves to our frames.Ý We hang on to them, even in tatters, because we donít think they can be replaced or we wonít find that level of comfort again.Ý We invest much time wearing them down like ocean waves soften beach glass, that they become as familiar as a family member. But in the case of Josephís red sweater vest, comfort and familiarity are only superficial reasons for his wearing it, because he will admit he has many equally comfortable, new sweater vests on the shelf, gifts from well meaning family members, which he doesnít prefer to wear.Ý Why? One could say the reason is a generational concept for his age group. Frugality, for those who experienced wartime, is a leftover notion created from ingrained habits of rationing, saving and using every scrap; the opposite ideology of our current ìthrow awayî society. Yet even with this added layer of explanation, there is still a much deeper meaning for this sweater.Ý For Joseph it represents the expected ìself denialî of a rigid Catholic upbringing, the welcoming of this denial on a subconscious level, a desire to be like Jesus with few meager possessions and taking very little of the world for himself.Ý The idea of sacrifice is a powerful spoken and unspoken message of Catholicism. Josephís religion permeates most of his thinking and actions even to the unconscious level. Although money is not a problem, he very rarely buys anything new; no lavish vacations, no expensive ìtoysî men are fond of, no fancy restaurants etc. Those who know him well attest to this.Ý He sacrifices even when itís beyond necessary to do so, without apparent self-awareness of it.Ý
ÝÝÝÝ It is very interesting to note, that although a father and grandfather, Joseph at one time aspired to be a priest, something long forgotten by him and his family.Ý Priests generally wear the same garments or robes; they strive to emulate the sacrifice of Jesus.Ý Josephís sweater, worn on an almost daily basis can be seen as a symbol of sacrifice and emulation of Priest/Jesus.Ý It is also ironic that the color of the sweater is red, like that of the Roman robe thrown on Jesus during his crucifixion or red like the ìblood of Christî.Ý At any rate this garment goes beyond our surface explanation of comfort, familiarity, beyond the socio-political concepts of post war survivors into a deeper spiritual subconscious representation of Joseph.
ÝÝÝÝ The rosary beads are old, and made of wood, blessed by a holy man. Joseph uses them several times daily, saying rosaries, novenas and special saint related prayers, which are the more complex prayer dogma of Catholicism. He goes beyond what most Catholics do, by making up lists of people to pray for in different categories; sick, dead, poor, dying, divorcing, political figures, sport teams etc.Ý If we look at the rosary beads and the obvious religious symbolism of such an item, we could be tempted to use the same explanation as the red sweater to define their significance, that of a deep spiritual, unconscious meaning. Subconsciously he desired to be a priest, rosary beads and frequent prayer are the domain of priest. These rosary beads are made of wood, symbolically the wood of the cross. But here, as with the sweater, the meaning goes much deeper.Ý
ÝÝÝÝ To discover this we need to question why does Joseph pray?Ý Is it to be a good Catholic or to emulate the priest he never was?Ý Is it because when faith is strong, people pray because they believe their prayers will be answered?Ý He does pray for these reasons, but this is only the superficial answer.Ý Underlying this is a deep psychological reason.Ý Joseph prays because he is afraid.Ý He lives in constant fear and always has.Ý Fear of death, illness, financial loss, robbery, murder, injury, fire, drowning, attacks, the worst of scenarios imagined, plague this man.ÝÝ A person who prays so fervently, so ìreligiouslyî should have the peace of mind one is said to get from prayer.Ý Joseph would never be described as a man with peace of mind.Ý He lives a life of extreme caution, a live of donít doís, a belief that the worst always happens, so better to not attempt something at all.Ý He fills himself on the bad news of the day, repeating it, believing in it as much as he does the doctrines and scriptures.Ý He spends a tremendous amount of time praying, hiding behind religion to avoid living.Ý Life and living involve some risk, some danger, for Joseph it is better to be the one doing the praying instead. To pray for everyone seems so noble, and in his mind it is because he does sincerely want to get divine help for his friends and family.Ý But he does not see why he is so driven to do it, and that it does not come from a peaceful place within.Ý Still, itís curious, people know of his prayer lists and will ask to be put on them.Ý They see him as a pious, quiet individual with his wooden rosary beads, and to some degree he is, but truthfully the religion is a mask for the fear underneath.Ý The red sweater can be seen as more of a true religious symbol for Joseph, as a subconscious emulation of Christ, then the rosary beads are.
ÝÝÝÝ The final item to be looked at is the black book, specifically used by Joseph to painstakingly log every medical detail of the last four terrible years of his wifeís life. He recorded medications, symptoms, vital signs, glucose levels, and insulin dosages.Ý His wifeís diabetes ravaged her body causing near blindness, organ damage, skin damage, multiple heart and circulatory crises. Doctors were amazed at the level of detail recorded that even they wouldnít attempt.Ý He spent hours doing this.Ý Partially this was a way to have some semblance of control over a devastating disease of a loved one.Ý But so much time devoted to some details that were irrelevant was overkill, and left little time to improve the emotional and mental health of his wife.Ý He attended faithfully to her basic needs like food, medications, trips to countless doctors etc.Ý But he never considered the emotional needs of his ìpatient.îÝ Intimacy was avoided by spending countless hours behind the black book.
ÝÝÝÝÝ The black book had been used throughout the years for assorted ìimportantî figures.Ý It was used for bookkeeping for bills, household expenses, careful logs of who owed him money, sport statistics, historical facts, and countless numbers, columns and bottom lines.Ý Joseph was a mathematical, statistical man by nature so it would seem natural for him to do so much record keeping.Ý But to his loved ones he was emotionally inaccessible.Ý When he wasnít praying he was immersed in logging detail. The black book was an impenetrable wall, a safe numerical barricade to keep busy behind.Ý It is the strongest representation of the psychological structure, organization and control he tried to have over himself and his life.Ý The effect the book had on him was like a black hole that swallows up all matter, so powerful was the draw.Ý Yet it never lets light escape, the light that illuminates a soul and opens them up to intimacy with other souls.Ý
ÝÝÝÝ It is an interesting ìonion peelî exercise to examine the significance of the metaphor represented in the ordinary objects of a personís life.Ý Each one like another jigsaw piece in a puzzle of a lifetime.Ý We can start to know a person through each of these odd shapes, a clue to the inner being.Ý We can learn a lot from a red sweater, wooden rosary beads and a black logbook.
Jane Schreck
WWII
House of Pain
House of pain, house of insane,
All described by a poet named Jane.
Wild eyes that donít see reality,
Eyes that want to put themselves shut,
Forever.
House on haunted hill ‚ the hauntings of the mind.
Catatonic, histrionic, stereophonic; all so ironic.
Halls echo with Vincent Price laughter or moans or voices or worse,
Silence.
Busy, busy, busy staff, busy putting you in order.
Square walls, square halls, communal stalls.
Pills against your will, or willingly thrill.
Your new home, home for a gnome, home alone.
They are all so
much sicker than me-
Why
am I here?Ý Why bother?Ý WhattteverrrÖ
Ugly colors, institutional, destitutional colors.
Look at all these kings horses, and women and men.
Can they put Humpty together again?
Leave me alone, or throw me a bone,
But donít make me look at my childhood home.
WaitÝ -Ý WaitÝ -Ý Wait
DigÝ -Ý DigÝÝ -Ý Dig
CryÝ -Ý CryÝ -ÝÝ Cry
Hope to DieÝ -DieÝ -Ý Die.
Or die to hope, hope on rope, cleaner than soap.
Cleaning the soul, making you whole,
If youíre lucky.
Jane Schreck
Writing Workshop II
2/24/01
ÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝÝ Beauty and the Beastie Boys
ÝÝÝÝ What is beauty to an American teenager?Ý
ÝÝÝÝ First, what is beauty? Beauty can be interpreted as that which pleases the senses.Ý What we find satisfying to mind, body and emotion.Ý Itís a circular process; we perceive beauty through visual, auditory and tactile medium that creates an emotional response we could describe as a ìbeautifulî feeling.Ý We achieve the intangible through the tangible.Ý The more intensely we perceive beauty the more intense the feeling; pleasure momentarily swells up in us like rising ocean waves.Ý People have been brought to tears of joy over what they consider beautiful.Ý Think of the exuberance of sports fan over a beautiful pass or slam dunk, or the opera enthusiast moved over a beautiful aria, or the art lovers rapture over a masterpiece or the joy of mother holding her beautiful newborn.Ý We are subjective creatures and so what we consider beautiful is purely personal.Ý We are divided on what essence we perceive as beautiful, our subjective choices, but we are united as human beings in the use of our mind and senses for the perception of beauty. We are influenced by common themes relative to our particular culture, gender or age group.Ý What an Australian Aborigine perceives as beauty is far different from a Japanese businessman or an American teenager.Ý
ÝÝÝÝ Beauty for an American teenager in the twenty first century has many influences. For many teenagers the concept of beauty has been force fed by a mass media. Their chameleon choices are the result of peer pressure, popular culture or parental influence.Ý Like their bodies, their tastes and sensibilities are constantly changing, underdeveloped and undiscovered. If beauty is defined as what is pleasing and satisfying and teenagers succumb to the popular notions of what is beautiful, what is really being manipulated is their concept of what is pleasing and satisfying.Ý This leads to a conflict between perceived beauty/pleasure versus true human sensations.Ý Take for example, getting multiple ear or body piercings and tattoos.Ý Strip away all the popular cultural and social satisfaction a teenager has with these and they may find getting pierced and tattooed an unsatisfying, painful experience.Ý The process of achieving the unrealistic emulation of the supermodel or Britney Spear-like icons is an unpleasant one if it leads to depression, anorexia or bulimia. These are examples in the visual/physical realm.Ý The other senses are involved too.Ý If we took popular teen music and peeled off the influential layers and teenagers listened purely from the human senses, they might find it unpleasantly loud or harsh. Even their taste buds are influenced by widely marketed fast food chains, candy and junk food companies. It is no wonder teenagers are conflicted when their perception of beauty, thus pleasure and satisfaction, are thwarted by popular dominant themes that cause new subliminal mantras like ìpain is goodî, ìphysical beauty at all costsî, ìloud, harsh, angry is okayî, or ìjunk food tastes bestî.
ÝÝÝÝ But even with all these influences, teenagers are subjective, individual creatures like the rest of humankind.Ý Perceptions of beauty along with all human perceptions are based on our own individual experiences with historical, cultural and social references.Ý Many try for uniqueness and originality, the teenager included.
ÝÝÝÝ So what exactly do teenagers find beautiful?Ý Is it different for girls and boys?Ý I decided to go right to the source by conducting some informal interviews of four teenagers via telephone.Ý I asked them what beauty is and to think about all the senses.Ý Here is what they had to say:
Nicole, age15:
ìHmm. Thatís a hard question. Itís how you see yourself. You decide whatís beautiful, what parts of yourself are beautiful.Ý I donít listen to what other people say, I try to be myself.Ý I like pictures of my friends and family because they remind me of the stuff we did, the good times.Ý I like candles and soft colors.Ý My room was white, then pink, then purple.Ý Now I want blues. I create my own space, my vision.Ý Oh yeah, and I like Momís Lladro statues, theyíre beautiful.Ý And paintings too. Itís what makes you feel good.Ý Animals are beautiful. I love my pets.Ý I love flowers, plants. Smells, like perfume, flowers, cooking, like, cooking apples.Ý I love my Plumeria cologne from Bath & Body works.Ý Sounds are important too.Ý I love music. Techno music.Ý Tastes arenít really beautiful, but fruit can look beautiful.îÝÝÝ
Chris, age 14:
ìItís physical, itís how you look.Ý But itís also whatís inside the person.Ý Itís artwork.Ý I like blues and greens for a room. I like a modern house.Ý I like to look at posters, like rock, girls, sports.Ý I like paintings, especially if you make the paintings.Ý Smells? Smells are beautiful, like cologne and perfume, fresh air and cooking food. Taste isnít beautiful. I like family pictures, pets.Ý Music is important. Beauty is feelings, internal.î
Kate Lynn, age 15:
ìBeauty is what you think about yourself.Ý You have an opinion, feelings. Itís girls in magazines, people on T.V. But itís inner and outer beauty.Ý I like to look at girls on TV, makeup, clothes, dresses. Certain kinds of music are beautiful. And smells like Cool Water or Tommy Hilfiger cologne.Ý Tastes are beautiful, yes, really, like, spaghetti or chicken.Ý Tastes can be really good.Ý In my room I like color, textures. I like light blue. I like posters of M & N, popular music stars, candles, incense, pictures of animals. Pets are beautiful. Nature is beautiful.Ý All animals are beautiful, water, birds, bees. I love nature. My family is my beauty.î
Timothy, age 16
ìI donít know, no one has ever asked me this before.Ý What is beauty?Ý It is the one thing that will always leave you breathless.Ý It can be anywhere, in a person, artwork. You have to see the whole.Ý Never look at one part.Ý A garden can look beautiful and smell beautiful.Ý Smells are beautiful like sweet smells or Italian cooking.Ý Tastes too, like your favorite food or desert or candy.Ý I just love the candy Swedish fish or lasagna.Ý Anything Italian. Music and voice are beautiful.Ý If you havenít heard from someone you love in a long time, their voice would be beautiful.Ý With music and voice beauty is not just in the person whoís performing but the listener too.Ý I love the song by Bon Jovi, ìItís My Life.î I love the words and how it makes me feel. As far as touch, textures, boys donít think about that as much as girls do.Ý I like colors.Ý Teenagers wear colors to reflect their personalities.Ý Thatís why you see so many teenagers wearing black, and I donít mean just the Goths. The Preppies wear bright blues and orange. I like dark blues or black.Ý Everybody wants to look different with their clothes and the colors they choose. Beauty can be physical, but itís much deeper.î
ÝÝÝÝÝ Itís a revealing exercise to compare some of their answers. All four teenagers related beauty with feelings and were able to use the different senses to detect beauty.Ý Some details were different but they touched on a common theme of beauty being internal.Ý They all mentioned blue in their color choice, could this be because teenagers feel the ìbluesî?Ý Is wearing black or other specific color significant on a deeper subconscious level?Ý All four found the smell of cooking food significant. Besides the basic hunger response, a deep feeling is triggered in our ìhome-connectionî psyche by the smell of cooking food.Ý Flowers, gardens and perfumes were mentioned, pure pleasure to most humans who arenít allergic. Not surprising, the girls mentioned name brands of perfumes; they are cosmetic company marketing targets, as all American women are.Ý Walking through any cosmetic department is like walking through a war zone; we dodge screaming visual torpedoes and cosmetic infantry ready to spray you with their perfume guns.Ý The teens differed on their opinion of taste. Curious that Nicole and Chris didnít consider taste as beautiful.Ý Teenagers are still growing physically; perhaps taste buds are the last to develop. Think of foods you considered detestable as a child or teen only to have acquired a taste for them later. I know very few children or teens, which consider olives, anchovies, liver or creamed spinach edible foods.Ý Most of them mentioned pets and animals as being beautiful.Ý Teenagers connect to their pets in a deeply emotional way.Ý The girls reflected more on visual and sensual as it related to their space, their room.Ý A room is particularly important to a teenage girl; they have a more developed sense of expression through decoration.
ÝÝÝÝ I asked the group to describe ugly the same way as they did beauty.Ý I asked them ìWhat is ugly?î Their comments surprised me:
Nicole:
ìNothing.Ý No, really. But plain, bare can be ugly.î
Chris:
ìIt can be physical, but itís more about an ugly personality.Ý Like when someone is a bitch or mean.î
ÝÝ
Kate Lynn:
ìNothing is ugly.Ý Itís all perception, opinion.î
Timothy:
ìUgly is something that makes you shiver. Going with the crowd is ugly.Ý People can have an ugly personality. Itís not really physical, butÖone time I saw this really overweight 13 year old girl in a tube top and tight pants, with way too much makeup. She was nasty.Ý Excess is ugly.î
ÝÝÝÝ I was astonished that the girls denied the existence of ugly, and that the boys gave much less detail than beauty.Ý Do they really feel this way?Ý Or were they trying to give altruistic answers?Ý If beauty feels satisfying, then ugly does not, and they would not want to dwell on the details.Ý Do feelings of ugliness get buried deep inside, pushed away and later expressed through drugs, alcohol, overeating etc.?Ý Timothy mentioned excess as being ugly.Ý Many teens go through mood swings and periods of depression.Ý Is this just hormonal or are buried ugly feelings more the culprit?Ý At any rate a true scientific study would have to be done to answer these questions.Ý The boys talked of ugly personalities.Ý Boys and men ridicule each other frequently under the guise of humor.Ý Male bonding toughens, female bonding nurtures.Ý All four gave their definition of ugly immediately in comparison to the pause and consideration they gave beauty.
ÝÝÝÝ Beauty for the American teenager is the feeling evoked through the evolving senses.Ý The choices, the details are subjective and individual, grown from experience and influenced by cultural, social and historical themes.Ý If it gives pleasure, ìtakes your breath awayî it is beautiful.Ý Beauty makes all of us feel good, even the teenager.Ý
Jane Schreck
WWII
(More bad poetry. Inspired by teenage self mutilations.)
Donít Try This At HomeÖ
I cut myself,
Because I loathe myself, Iím ugly and dirty.
I cut myself,
Because I hate you for not seeing the monster.
I cut myself,
Because I hate and love the monster/angel/monster.
I cut myself,
Because I hate myself for upsetting all the apple carts.
I cut myself,
Because I hate the clueless who think they can help.
I cut myself,
Because I hate this place and I want to go home.
I cut myself,
Because I like to see how the pain on the inside looks on the outside.
I cut myself,
Because I canít feel anything.
I cut myself,
Because I like it,
and you canít stop me.